LSU Health New Orleans School of Medicine New Orleans, LA
Stephany Nguyen, MD, Seth Vignes, MD LSU Health New Orleans School of Medicine, New Orleans, LA Introduction: The three main etiologies of liver abscesses are infectious, malignancy, or iatrogenic. This highlights a case where a large biliary stone, initially concerning for malignancy on imaging, resulted in liver abscesses due to an atypical obstruction.
Case Description/
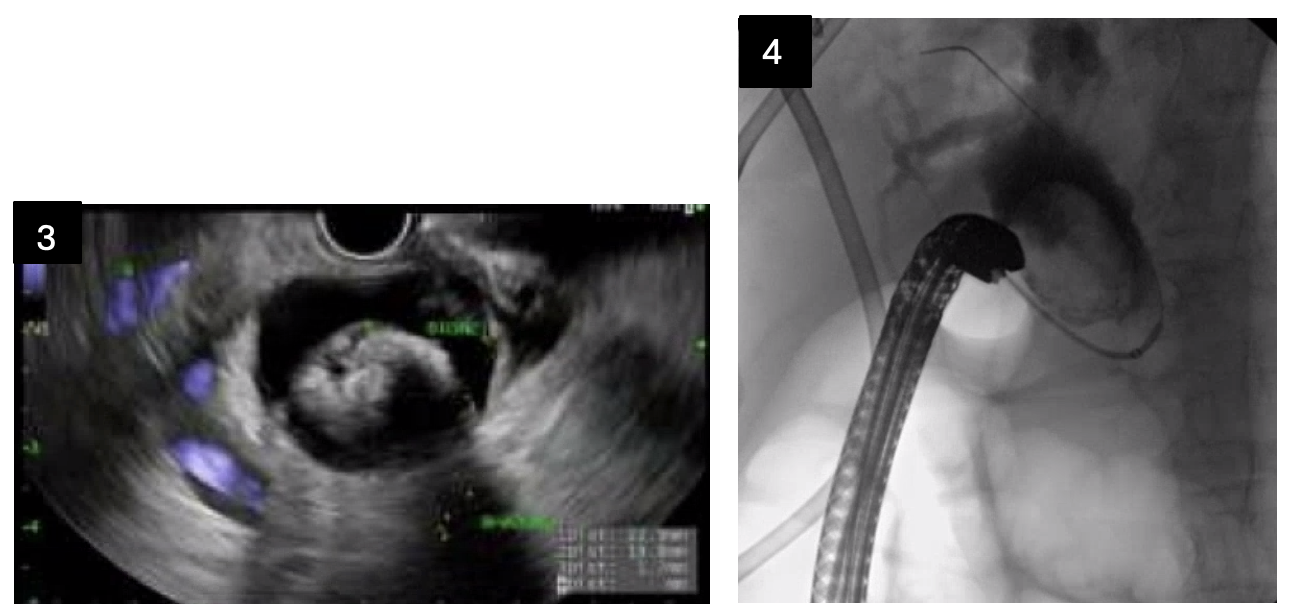
Methods: A 75-year-old female with a history of cholecystectomy in 2000 presented with right upper quadrant abdominal pain and fever for two weeks. CT abdomen and MRCP revealed two 3-4 cm complex cystic foci in the liver concerning for abscesses, diffuse intra and extrahepatic ductal dilation, and a 3 cm complex low-density focus near the duodenum concerning for enlarged lymph nodes or malignancy. She had normal transaminases, bilirubin, CEA, and CA 19-9. The liver abscesses were drained and treated with four weeks of Augmentin based on cultures that grew Citrobacter and Proteus. Subsequent EUS revealed a 22 mm stone in the middle one-third of the bile duct, and no masses were noted in the region seen on MRCP. She underwent ERCP the following day with lithotripsy for stone fragmentation. However, removal of the largest stone was incomplete as part of it was lodged in a lateral outpouching of the common bile duct. She was started on ursodiol and followed up outpatient for serial ERCPs with stent exchanges and lithotripsy. All subsequent biliary imaging showed persistent common bile duct lateral outpouching with indwelling stone. Discussion: Infectious liver abscesses are usually a result of biliary tract obstruction, such as stones, strictures, and malignancy. In this case, our patient’s initial imaging was concerning for malignancy resulting in biliary obstruction. However, there were no endosonographic abnormalities on EUS other than a 22 mm stone and sludge. Interestingly, after serial ERCPs for removal of the large stones, the bile duct remained dilated up to 19 mm, but the lesion near the pancreatic head was no longer identified on repeat CT abdomen. Current consensus from the medical team is this finding was the lateral bile duct outpouching with large, indwelling stone, which was partially improved with lithotripsy. Repeat EUS is scheduled for re-evaluation of that area.
Figure: Figure 1: CT abdomen with 3.4 x 2.7 cm foci near duodenum. Figure 2: Repeat CT abdomen several months later with mass effect attenuated after lithotripsy and biliary stent placement.
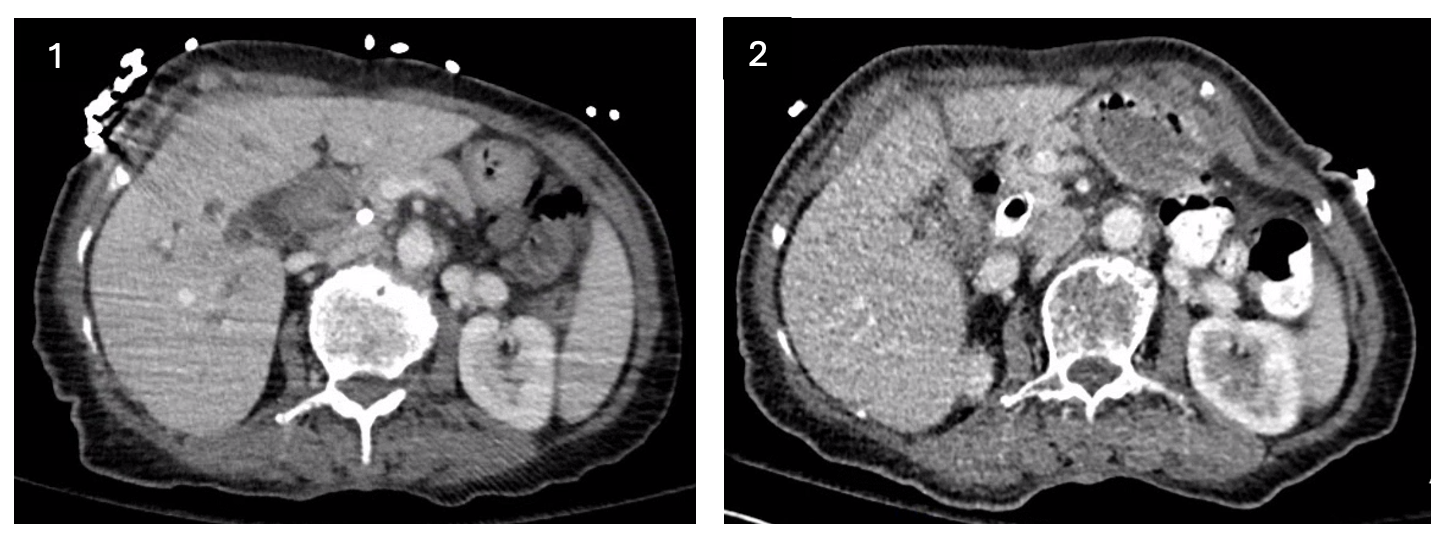
Figure: Figure 3: Initial EUS with large gallstone in bile duct. Figure 4: ERCP revealing stone outside of the bile duct.
Disclosures: Stephany Nguyen indicated no relevant financial relationships. Seth Vignes indicated no relevant financial relationships.
Stephany Nguyen, MD, Seth Vignes, MD. P4452 - Bile Duct Outpouching With Large Gallstone Resulting in Obstruction and Liver Abscesses, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.