Nicole Villa, MD1, Oscarina Gonzalez, MD1, Julio C. Valencia-Manrique, MD1, Carla Barberan Parraga, MD2, Jennifer Harley, MD1 1NYC Health + Hospitals/Metropolitan, New York, NY; 2Maimonides Medical Center, Brooklyn, NY Introduction: Choledochal cysts are uncommon congenital anomalies of the biliary system and are usually diagnosed in childhood. When these lesions present later in life, the symptoms are often vague, and diagnosis may be delayed. Among the different types, type I cysts may lead to cholangitis, pancreatitis, or malignancy if not recognized. This case describes a young adult initially thought to have a biloma, whose workup revealed a type I choledochal cyst (T1CC).
Case Description/
Methods: A 26-year-old woman with a history of cholecystectomy presented with abdominal pain. Labs showed hyperbilirubinemia (total bilirubin 2.3 mg/dL, direct 1.9 mg/dL), elevated ALT (468 U/L), AST (308 U/L), and alkaline phosphatase (186 U/L). Initial CT revealed a 6.8 × 7.4 × 9.7 cm cystic collection at the porta hepatis level, causing mass effect on the duodenum and pancreas, without clear communication with the biliary tree and no biliary ductal dilation. A follow-up HIDA scan demonstrated no radiotracer passage into the duodenum but progressive uptake within a rounded structure at the porta hepatis. IR drainage was attempted but was unsuccessful. The patient improved clinically and was discharged after five days. One month later, she returned with recurrent symptoms. Repeat CT showed enlargement of the collection and increased mass effect. Successful IR drainage was performed, but persistent high output raised concern for bile leak. ERCP showed fusiform dilation of the common bile duct with a large cystic cavity containing the percutaneous drain, consistent with a T1CC. A biliary stent was placed. MRCP showed interval decrease in the size of the cystic lesion following drainage and demonstrated communication with the common hepatic and common bile ducts, consistent with a T1CC. The patient later underwent a Whipple procedure. Discussion: T1CCs can resemble acquired conditions like bilomas, especially post-cholecystectomy. In this case, HIDA suggested a bile leak, while MRCP provided clearer anatomic detail, revealing a congenital ductal anomaly. MRCP offers high sensitivity and specificity for biliary tract abnormalities and is preferred for evaluating structural lesions. This highlights its diagnostic value when standard imaging is inconclusive or misleading. Clinicians should consider congenital etiologies like T1CC in adults with unexplained cystic biliary lesions, particularly when initial interventions fail to resolve symptoms. Timely diagnosis is essential to avoid repeated procedures and to guide surgical treatment.
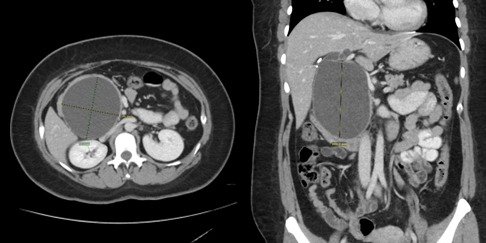
Figure: Repeat CT Abdomen showing an enlarging cystic lesion 9.2x8.5x10.5cm extending from the porta hepatis to the pancreatic head, with associated intrahepatic biliary ductal dilation and mass effect on the inferior vena cava
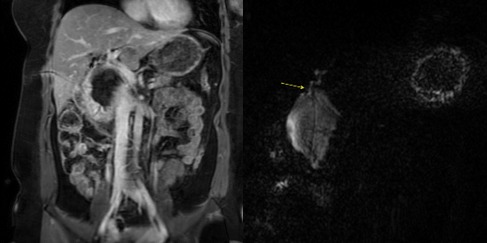
Figure: MRCP showing interval decrease in the size of the cystic lesion status post percutaneous drainage, with evidence of communication with the common hepatic duct and common bile duct
Disclosures: Nicole Villa indicated no relevant financial relationships. Oscarina Gonzalez indicated no relevant financial relationships. Julio Valencia-Manrique indicated no relevant financial relationships. Carla Barberan Parraga indicated no relevant financial relationships. Jennifer Harley indicated no relevant financial relationships.
Nicole Villa, MD1, Oscarina Gonzalez, MD1, Julio C. Valencia-Manrique, MD1, Carla Barberan Parraga, MD2, Jennifer Harley, MD1. P4442 - A Surprising Turn: Type I Choledochal Cyst Uncovered Amidst Treatment for Suspected Biloma, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")