Bushra Bangash, MD1, Aakriti Soni, MD2, Galvin S. Dhaliwal, MD2, Ahmed Ouni, MD3 1HCA Gulf Coast Division - - Texas City, TX, Spring, TX; 2HCA Healthcare Kingwood Hospital/University of Houston, Houston, TX; 3HCA Healthcare Kingwood Hospital/University of Houston, Kingwood, TX Introduction: Mirizzi syndrome is a rare but important complication of chronic gallstone disease, affecting about 0.05–2.7% of patients. It results from a stone impacted in the cystic duct or gallbladder neck that compresses the common hepatic duct. In Type I, this causes external compression without a fistula. Traditionally, open cholecystectomy has been the preferred treatment. Laparoscopic cholecystectomy is sometimes attempted but has a 41% risk of conversion due to inflammation and distortion near Calot’s triangle. Endoscopic approaches have emerged as less invasive options in selected cases. We present a case of Type I Mirizzi syndrome successfully treated with SpyGlass-guided electrohydraulic lithotripsy (EHL).
Case Description/
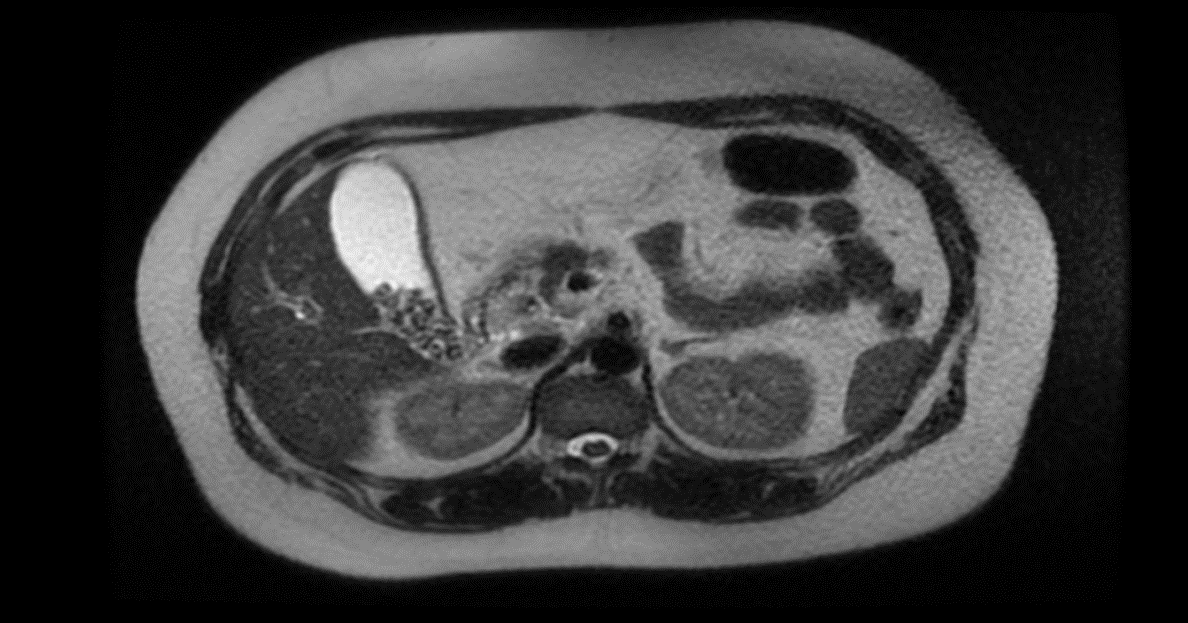
Methods: A 28-year-old woman with no significant medical history presented with two days of constant right upper quadrant pain radiating to the back, preceded by two weeks of intermittent discomfort. On exam, she was afebrile, stable, and had a positive Murphy’s sign. Initial labs showed elevated liver enzymes: aspartate aminotransferase (AST) 158 U/L and alanine aminotransferase (ALT) 101 U/L. By the next day, her labs had worsened—AST rose to 1022 U/L, ALT to 752 U/L, and total bilirubin increased to 1.6 mg/dL. Ultrasound revealed a 6.6 mm dilated common bile duct with gallstones at the gallbladder neck. Magnetic resonance cholangiopancreatography (MRCP) showed a 9 mm filling defect at the junction of the cystic duct and bile duct, suggestive of Mirizzi syndrome. Endoscopic retrograde cholangiopancreatography (ERCP) confirmed a 15 mm impacted stone in the cystic duct compressing the hepatic duct. SpyGlass cholangioscopy allowed direct visualization, and EHL was used to fragment and remove the stone in one session. A repeat ERCP two days later to retrieve a stent that was originally placed for decompression, confirmed resolution. The patient was discharged in stable condition. Discussion: This case illustrates how advanced endoscopic tools like SpyGlass can provide effective, minimally invasive treatment for Mirizzi syndrome Type I. Direct visualization enables precise lithotripsy, reducing the need for surgery in select patients. For those with significant inflammation or complex anatomy, this approach offers a safe and efficient alternative with low complication risk.
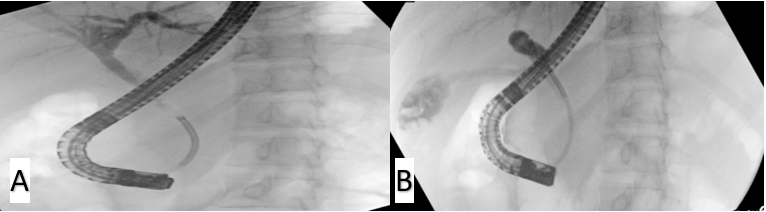
Figure: Figure 2: A: Filling defect seen in cholangiogram during ERCP. B: Final ERCP showing filling defect resolved after SpyGlass-guided lithotripsy
Disclosures: Bushra Bangash indicated no relevant financial relationships. Aakriti Soni indicated no relevant financial relationships. Galvin Dhaliwal indicated no relevant financial relationships. Ahmed Ouni indicated no relevant financial relationships.
Bushra Bangash, MD1, Aakriti Soni, MD2, Galvin S. Dhaliwal, MD2, Ahmed Ouni, MD3. P4436 - SpyGlass-Guided Electrohydraulic Lithotripsy: A Brighter Future for Mirizzi's Syndrome Management, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.