University of Kentucky Chandler Medical Center Lexington, KY
Ujasbhai Patel, MD1, Rebecca Aquino, MD1, Kshitij Thakur, MD2 1University of Kentucky College of Medicine, Lexington, KY; 2University of Kentucky, Lexington, KY Introduction: In a typical case of acute cholecystitis, performing a cholecystectomy results in the resolution of underlying symptoms in 95% of patients. The other 5% of patients have atypical origins for case presentation that may be underdiagnosed. Intraductal papillary neoplasm of the bile duct (IPNB) can present with vague abdominal symptoms and can occasionally be asymptomatic with diagnosis revealed through ERCP. Herein, we present the case of a relatively healthy elderly patient with IPNB manifesting with cholecystitis.
Case Description/
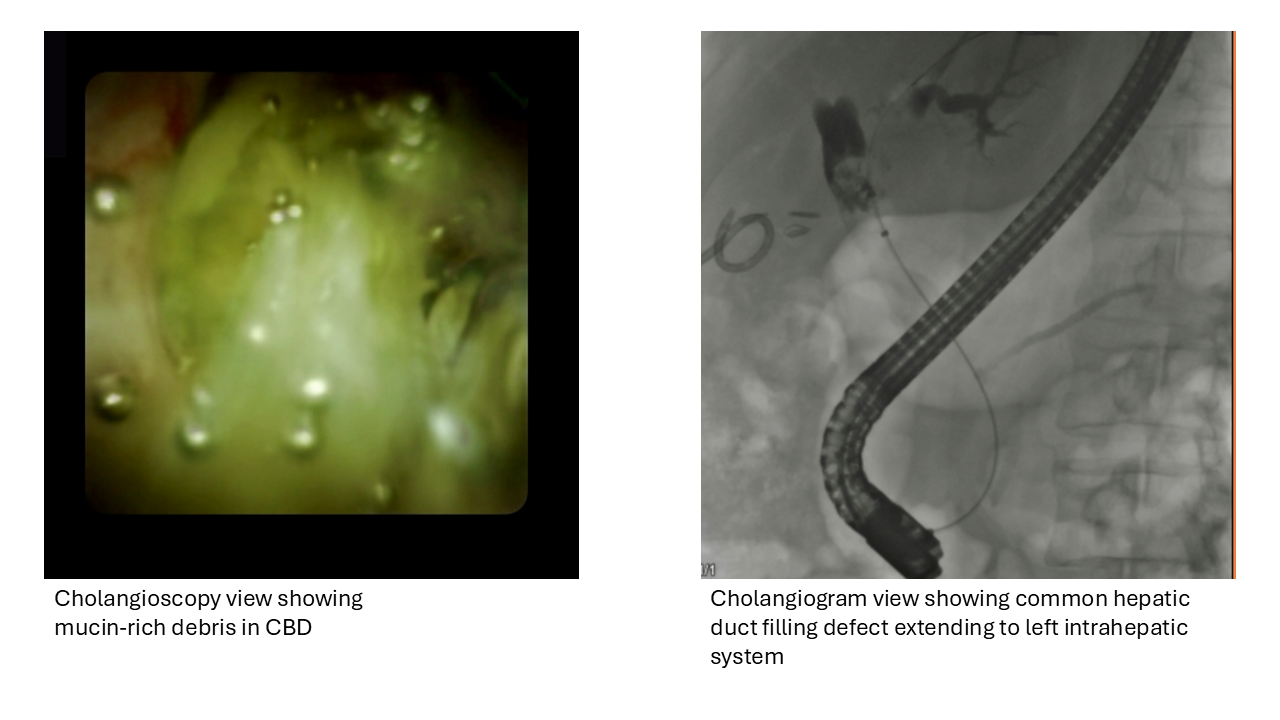
Methods: A 71-year-old male with no significant history related to the case presents with right-sided abdominal pain and fever for 3 days. He has mixed pattern of liver injury with AST and ALT elevated twice the upper limit of normal and total bilirubin of 1.2. The patient is found to have acute cholecystitis by sonography and in accordance, he underwent cholecystectomy. The intraoperative cholangiogram revealed a possible filling defect. Magnetic Resonance Cholangiopancreatography (MRCP) was recommended. This showed a 12 cm complex fluid collection at the common hepatic duct (CHD) and near segment 4 of the liver thought to represent an abscess. The common bile duct (CBD) was diffusely dilated. There was a direct communication from the cystic mass with the dilated biliary tree. Per radiology, while this could represent a ruptured abscess, intraductal biliary neoplasm should be considered. A drain was placed into the fluid collection and infectious studies were all negative. Due to diffuse left intrahepatic dilation, an ERCP was suggested. ERCP was met with expression of mucin-rich debris on biliary sweep after sphincterotomy. Cholangiogram showed a 2 cm complete filling defect of CHD and left intrahepatic. Cholangioscopy confirmed adherence of thick mucin restricted to this area. SpyBite biopsies confirmed IPNB with high-grade dysplasia. The patient underwent extrahepatic bile duct excision along with left trisegmentectomy and Roux-en-Y hepaticojejunostomy. The final surgical pathology diagnosis was invasive metastatic adenocarcinoma arising from IPNB. Unfortunately for the patient, there was post-op disease progression and thus, further immunotherapy will be required. Discussion: We present an interesting case with a rare type of presentation for IPNB as acute cholecystitis with subsequent ERCP reliably revealing the diagnosis. Clinicians should be cognizant of atypical presentations for cholecystitis as the treatment for the underlying etiology may differ drastically.
Figure: Cholangioscopy and cholangiogram views of the suspect IPNB
Disclosures: Ujasbhai Patel indicated no relevant financial relationships. Rebecca Aquino indicated no relevant financial relationships. Kshitij Thakur indicated no relevant financial relationships.
Ujasbhai Patel, MD1, Rebecca Aquino, MD1, Kshitij Thakur, MD2. P4400 - Intraductal Papillary Neoplasm of the Bile Duct as a Rare Underlying Etiology to Acute Cholecystitis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.