University of Illinois College of Medicine Peoria, IL
Ankita Nekkanti, MD, Navjit Singh, MD, Jason Bill, MD University of Illinois College of Medicine, Peoria, IL Introduction: Secondary hepatic involvement by diffuse large B-cell lymphoma (DLBCL) is uncommon and rarely the initial disease manifestation. When present, it can mimic primary hepatobiliary malignancies clinically and radiographically. We report a case of secondary hepatic DLBCL presenting with obstructive jaundice and a central liver mass, initially presumed to be cholangiocarcinoma.
Case Description/
Methods: A 69-year-old man presented with nausea, dark urine for one week, and right hip pain for three months. He had a history of stage I, grade 1 follicular lymphoma localized to the left neck, treated with radiation one year prior, with post-treatment positron emission tomography (PET) showing only post-radiation changes. On admission, labs revealed a cholestatic liver enzyme pattern and direct hyperbilirubinemia of approximately 17 mg/dL. Computed tomography (CT) abdomen demonstrated a central hepatic mass with intrahepatic biliary dilation, concerning for cholangiocarcinoma. CA 19-9 was markedly elevated. Imaging also showed lytic lesions in multiple ribs, and the right iliac wing, as well as retroperitoneal lymphadenopathy. Multiple endoscopic retrograde cholangiopancreatographies (ERCPs) revealed a malignant-appearing hilar stricture; intrahepatic stents were placed, resulting in modest bilirubin improvement. Brushings and biopsies from the stricture failed to yield sufficient tissue for diagnosis. After two months of progressive hyperbilirubinemia and no definitive diagnosis, an ultrasound-guided biopsy of the liver mass was pursued, which revealed DLBCL, germinal center B-cell subtype. He was started on R-CHOP chemotherapy (rituximab, cyclophosphamide, doxorubicin, vincristine, prednisone), leading to rapid bilirubin decline. After six cycles, PET scan showed significant treatment response. Discussion: Transformation of follicular lymphoma into aggressive lymphoma such as DLBCL occurs at a rate of 2–3% per year and carries a worse prognosis. In this case, the liver mass, biliary obstruction, and elevated CA 19-9 led to a presumed diagnosis of cholangiocarcinoma. However, bone lesions—uncommon in cholangiocarcinoma—should have prompted earlier reconsideration of the differential. While ERCP was appropriate, repeated nondiagnostic sampling delayed tissue confirmation. Alternative biopsy approaches, including percutaneous liver or bone lesion biopsy, may have expedited treatment. This case highlights the risk of diagnostic anchoring and the importance of integrating all clinical and imaging findings.
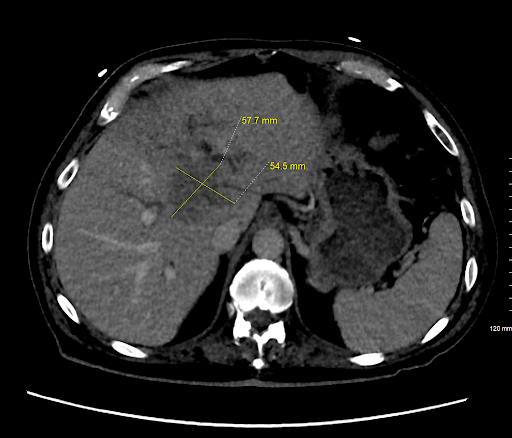
Figure: CT Abdomen showing large central hepatic mass with upstream intrahepatic biliary dilation.
Figure: Biopsy of liver mass showing diffuse proliferation of large, atypical lymphoid cells with large nuclei and prominent nucleoli.
Disclosures: Ankita Nekkanti indicated no relevant financial relationships. Navjit Singh indicated no relevant financial relationships. Jason Bill indicated no relevant financial relationships.
Ankita Nekkanti, MD, Navjit Singh, MD, Jason Bill, MD. P4394 - Secondary Diffuse Large B-Cell Lymphoma Mimicking Cholangiocarcinoma, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.