Divya Roy, DO, Murad H.. Ali, MD, Suryanarayana Reddy Challa, MD, Jessica Widmer, DO NYU Langone Health, Mineola, NY Introduction: Ketamine is a rarely reported cause of pancreatitis. While ketamine may exert some opioid receptor activity that could contribute to sphincter of oddi dysfunction, this mechanism has not been well studied in human models. We describe the case of a 23 year old male with a five month history of recreational ketamine use who presented with painless obstructive jaundice. To our knowledge this is the first reported case of ketamine induced chronic pancreatitis radiographically mimicking autoimmune pancreatitis, with the diagnosis excluded through histopathologic evaluation.
Case Description/
Methods: A 23 year old male with no significant past medical history and a 5 month history of ketamine use was referred to the emergency department from his primary care physician for evaluation of a two week history of painless jaundice, pale stools, and dark urine. An abdominal ultrasound revealed severe intra-hepatic and biliary ductal dilation with a distended gallbladder, but no gallstones or signs of acute cholecystitis were noted.
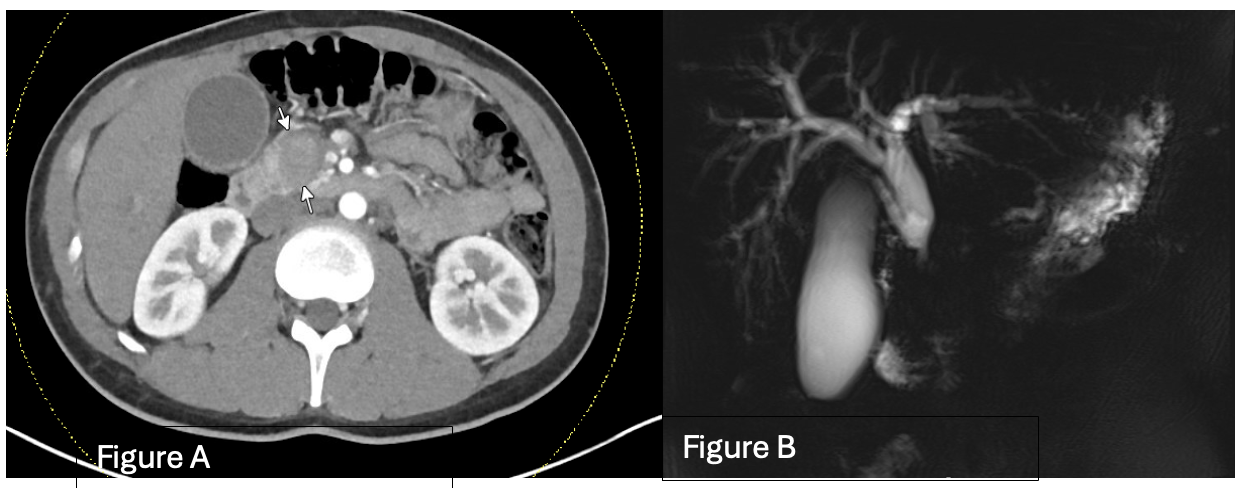
Initial laboratory studies showed a total bilirubin of 14 mg/dL, direct bilirubin of 11 mg/dL, alkaline phosphatase of 302 U/L, AST of 51 U/L, ALT 79 U/L, lipase of 103, Ca 19 < 1, CEA 2.6 and an Ig level of 1,193 within normal limits. Cross sectional imaging including CT pancreas and MRCP demonstrated a 4 by 6 cm mass in the head of the pancreas with radiographic features of autoimmune pancreatitis.
The patient underwent endoscopic ultrasound with fine needle aspiration (EUS-FNA) and endoscopic retrograde cholangiopancreatography (ERCP) with biliary stent placement, resulting in improvement in liver function tests and symptoms. Histopathology from the FNA ruled out autoimmune pancreatitis, revealing chronic pancreatic inflammation without plasma cell infiltration. The patient was advised to discontinue ketamine use, and he underwent stent removal and is currently without symptoms. Discussion: Ketamine has not been widely reported as a cause of pancreatitis and is not well studied to establish a definitive causal relationship. To date, only one published case has described ketamine-associated sphincter of oddi dysfunction requiring sphincterotomy. In our case, the patient's clinical improvement following cessation of ketamine use supports a potential association between ketamine and pancreatic inflammation. While further research is needed, ketamine should be used with caution or avoided entirely as an analgesic in patients with a history of pancreatitis.
Figure: Figure A: CT Pancreas with arrows pointing to a heterogenous mass at the head of pancreas Figure B: MRCP Cholangiogram showing severe CBD dilation, gallbladder distention and pancreatic obstruction at the head
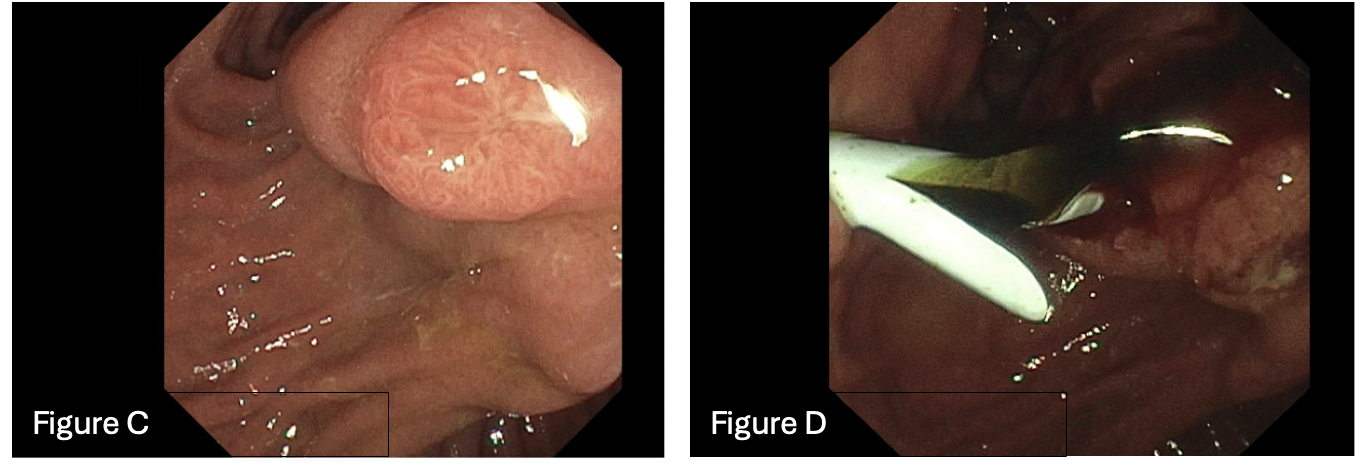
Figure: Figure C: ERCP imaging of duodenal ampulla bulging Figure D: ERCP imaging post ductal stent placement with good drainage of bile
Disclosures: Divya Roy indicated no relevant financial relationships. Murad Ali indicated no relevant financial relationships. Suryanarayana Reddy Challa indicated no relevant financial relationships. Jessica Widmer indicated no relevant financial relationships.
Divya Roy, DO, Murad H.. Ali, MD, Suryanarayana Reddy Challa, MD, Jessica Widmer, DO. P4383 - An Unusual Case of Chronic Pancreatitis Secondary to Recreational Ketamine Use, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")