Fares Jamal, MD1, Astin Worden, MD1, Kornpong Vantanasiri, MD2, Irving Jorge, MD1, Terry L.. Jue, MD3, Michelle A.. Anderson, MD1 1Mayo Clinic, Phoenix, AZ; 2Mayo Clinic Arizona, Phoenix, AZ; 3Mayo Clinic Arizona, Scottsdale, AZ Introduction: Mirizzi syndrome is a rare complication of cholelithiasis caused by an impacted stone in the cystic duct or gallbladder neck compressing the adjacent common hepatic duct. Chronic inflammation and pressure can lead to erosion and fistula formation between the cystic duct and the common bile duct (CBD). These fistulas are rare and often not diagnosed until surgery, as they may mimic other causes of biliary obstruction.
Case Description/
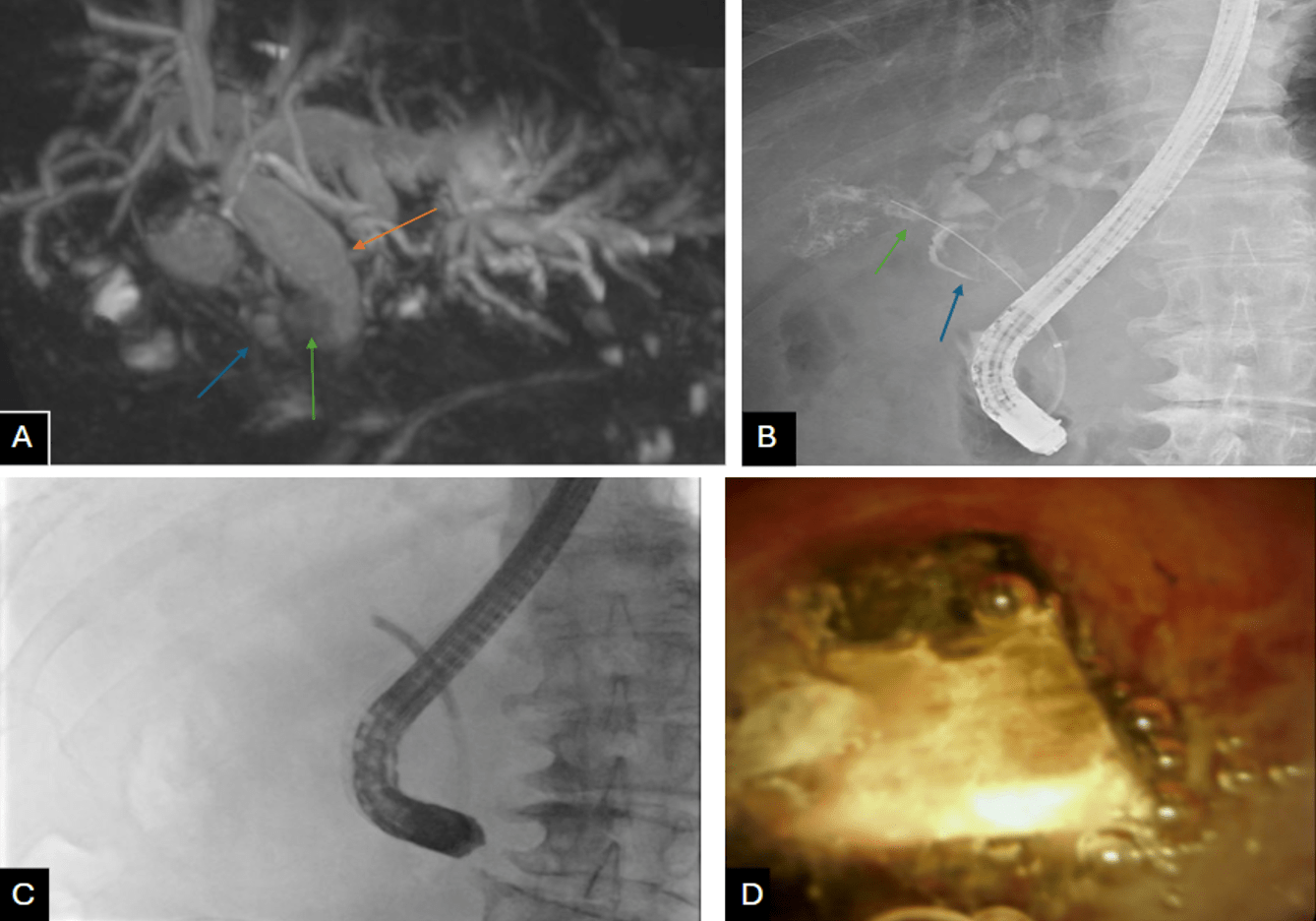
Methods: A 77-year-old male with COPD, ulcerative colitis, and 10-year history of asymptomatic cholelithiasis presented with right upper quadrant pain and obstructive jaundice. Labs showed T bili 5.3, D bili 3.5, AST 80, ALT 166, ALP 662. MRCP revealed at least 4 large gallstones, measuring up to 2.1 cm, with the distal stone within the cystic duct at the confluence of the CBD, resulting in proximal CBD dilatation up to 1.7cm, suggestive of Mirizzi Syndrome (Image A). He underwent robotic assisted subtotal cholecystectomy and CBD exploration, but the impacted stone could not be retrieved. Intraoperative ERCP revealed common hepatic duct stricture due to suspected extrinsic compression and a cystic duct leak (Image B). A biliary sphincterotomy was completed, and a 10 F x 10 cm plastic stent was placed with proximal end above the stricture and cystic duct takeoff. Cholangioscopy performed on subsequent ERCP (Image C) revealed a fistulous tract between the remnant cystic duct and bile duct with ulcerated mucosa surrounding the impacted stone. After serial ERCPs with extensive electrohydraulic lithotripsy (EHL), the remaining impacted CBD stone fragment was small enough to permit excellent biliary drainage. The patient did well on a stent-free trial with normalization of LFTs and resolution of abdominal pain. Discussion: This case highlights an advanced variant of Mirizzi syndrome where chronic inflamamtion and direct compression from the stone lead to a cystic duct–CBD fistula. Preoperative diagnosis is challenging and is often made intraoperatively or on fluoroscopy and cholangioscopy as seen in this case. Management depends on the extent of the fistula and bile duct involvement. It ranges from endoscopic stenting to biliary reconstruction depending on the severity of the fistula and the extent of bile duct damage. In this case, the fistulous tract was small and able to resolve with EHL and serial stenting. This case highlights the importance of a multidisciplinary approach and diligent follow-up to detect complications.
Figure: A) MRCP demonstrating impacted stone (green arrow) within the cystic duct (blue arrow) impinging upon the common bile duct resulting in upstream dilatation (orange arrow). B) Cholangiogram with contrast extravasation from the cystic duct stump (green arrow), impacted cystic duct stone (blue arrow) C) Cholangiogram view of SpyGlass probe at the level of the fistula D) Spyglass view at the opening of the fistula.
Disclosures: Fares Jamal indicated no relevant financial relationships. Astin Worden indicated no relevant financial relationships. Kornpong Vantanasiri indicated no relevant financial relationships. Irving Jorge: Boston Scientific Corporation – Grant/Research Support. Terry Jue: Boston Scientific – Jan 2024, Honorarium received for serving as an Instructor at Fellows' Tissue resection course. Michelle Anderson: Boston Scientific – Consultant.
Fares Jamal, MD1, Astin Worden, MD1, Kornpong Vantanasiri, MD2, Irving Jorge, MD1, Terry L.. Jue, MD3, Michelle A.. Anderson, MD1. P4381 - From Obstruction to Fistula: A Rare Presentation of Mirizzi Syndrome Managed Endoscopically, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.