Neal K. Bhachawat, DO1, Zara Ijaz, MD1, Bradley D. Adams, MD2, Yahor Sukharutski, MD1 1Houston Methodist Hospital, Houston, TX; 2Houston Methodist-Weill Cornell Graduate School of Medical Sciences, Houston, TX Introduction: Meckel’s diverticulum (MD), the most common congenital gastrointestinal tract anomaly, is a true diverticulum typically located near the ileocecal valve. It affects about 2% of the population, but complications are rare, occurring in only 4–7% of cases. Perforation is especially uncommon. We present a case of perforated MD in a young adult initially misdiagnosed due to nonspecific symptoms and unremarkable early imaging.
Case Description/
Methods: A 22-year-old woman with a history of irritable bowel syndrome presented with 4 days of sharp, constant right lower quadrant abdominal pain, nausea, vomiting, and decreased appetite. She denied fever, bowel or urinary changes, and was not sexually active. A CT abdomen/pelvis (A/P) with IV contrast done 2 days earlier was unremarkable. On arrival, she had sinus tachycardia (HR 120s) and right lower quadrant tenderness with guarding. Labs showed hypokalemia (2.8 mEq/L) and non-anion gap metabolic acidosis. Serum Beta HCG and STD testing (HIV, Syphilis, Chlamydia and Gonorrhea) were negative. Complete blood count was unremarkable. Pelvic ultrasound showed pelvic free fluid with hemorrhagic/proteinaceous debris. OB/GYN evaluation favored a ruptured hemorrhagic ovarian cyst. Her pain persisted, prompting repeat CT A/P with IV contrast, which showed a pelvic fluid and gas collection (3.4 x 2.9 cm) abutting multiple bowel loops, concerning for perforated viscus (image 1). Same day repeat CT A/P with IV and oral contrast showed contrast along a small bowel loop diverticulum, contiguous with the lower pelvic collection, suspicious for perforated Meckel's diverticulitis with abscess formation (image 2). She underwent urgent laparoscopy with removal of a gangrenous, perforated MD and intra-abdominal abscess drainage. Intra operative pathology showed no ectopic tissue or malignancy and cultures grew Alpha Streptococcus and Bacteroides ovatus. Blood cultures remained negative. She was discharged on ciprofloxacin and metronidazole for 5 days with symptom resolution. Discussion: MD is often misdiagnosed due to its rarity and vague symptoms. Even contrast-enhanced CT may miss the diagnosis. This case highlights the diagnostic challenge of complicated MD and the value of maintaining clinical suspicion despite negative imaging. Repeat CT with oral contrast proved critical in localizing the leak and guiding surgical management. Exploratory laparoscopy remains key in unclear acute abdominal presentations.
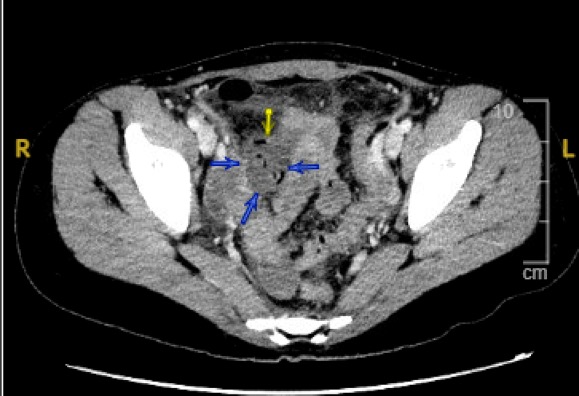
Figure: Image 1: Compute Tomography (CT) abdomen/pelvis with intravenous contrast axial view showing the collection of fluid and gas (3.4 x 2.9 cm) abutting the small bowel in the right lower quadrant. Unclear site of perforation but highly concerning for perforated viscus.
Figure: Image 2: Compute Tomography (CT) abdomen/pelvis with intravenous and enteric contrast axial view showing a blind-ending diverticulum coming off of the ileum in the region of this fluid/gas collection.
Disclosures: Neal Bhachawat indicated no relevant financial relationships. Zara Ijaz indicated no relevant financial relationships. Bradley Adams indicated no relevant financial relationships. Yahor Sukharutski indicated no relevant financial relationships.
Neal K. Bhachawat, DO1, Zara Ijaz, MD1, Bradley D. Adams, MD2, Yahor Sukharutski, MD1. P1959 - Perforated Meckel’s Diverticulum in a Young Adult: A Diagnostic Challenge in Acute Abdomen, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.