Shiv R. Patel, MD1, Hari Movva, MD2, Lucia Soca Gallego, DO2, Mahnur Haider, MD2, Sreeram Parupudi, MD2 1University of Virginia, Charlottesville, VA; 2University of Texas Medical Branch, Galveston, TX Introduction: Hepatocellular carcinoma (HCC) is the fourth highest cause of cancer-associated mortality in the world. HCC metastasis to the heart is rare and associated with a poor prognosis. Here, we present a case of HCC with tumor involvement of the right atrium and inferior vena cava (IVC) at the time of initial diagnosis. Involvement of the atrial structures is seen in less than 4% of all HCC cases.
Case Description/
Methods: A 65-year-old female with hepatitis C cirrhosis presented with 2 months of epigastric pain. On examination, she had mild epigastric tenderness and bilateral leg swelling. Labs revealed an elevated alpha-fetoprotein of 309 ng/mL and Model for End-Stage Liver Disease (MELD) 3.0 score of 27 points. Magnetic resonance imaging (MRI) of the abdomen showed a cirrhotic liver with a 6.5 cm right hepatic lobe mass extending into the right hepatic vein, IVC, and right atrium. The imaging findings were diagnostic for HCC considering the Liver Imaging Reporting and Data System (LI-RADS) score was 5. Transthoracic echocardiogram revealed a fixed, echogenic spherical mass measuring 4.7 × 5.5 cm, consistent with intracardiac tumor thrombus. Given the extent of the disease, she was not a candidate for surgical resection or liver transplantation. She began systemic therapy along with stereotactic body radiation therapy (SBRT), but had minimal response. Less than four months after diagnosis, she experienced sudden cardiac arrest and died. The clinical course was consistent with a malignant arrhythmia as the cause of death. Discussion: Cardiac involvement in HCC is rare and associated with a high mortality, with median survival of 1–4 months despite treatment. While intracardiac HCC often causes mechanical issues like IVC obstruction, tumor invasion of myocardial or conduction tissue can trigger fatal arrhythmias. Metastatic cardiac tumors have been associated with atrial fibrillation, heart block, and ventricular arrhythmias, occasionally leading to sudden cardiac arrest.
This case highlights two key considerations: cardiac arrest in intracardiac HCC may result from malignant arrhythmia, not just mechanical obstruction; and SBRT, while a palliative option, may be insufficient and pose cardiac risks. Early rhythm monitoring and cardiology involvement should be considered, even without symptoms. Further research is needed to better understand arrhythmia risk and SBRT cardiotoxicity in this setting.
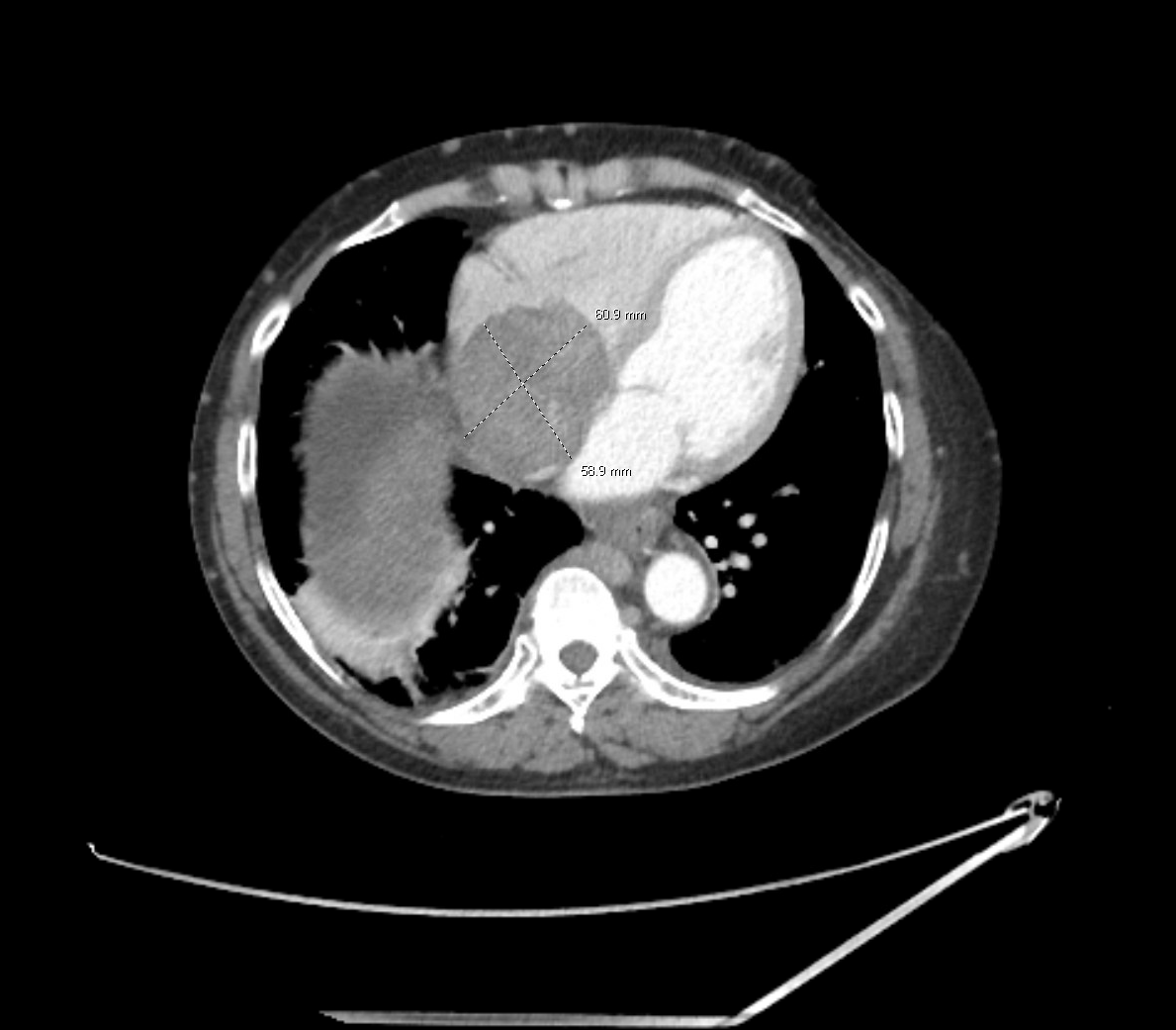
Figure: A computed tomography scan revealing an approximately 6.0 × 6.0 cm lesion extending into the right atrium from the patient’s underlying HCC.
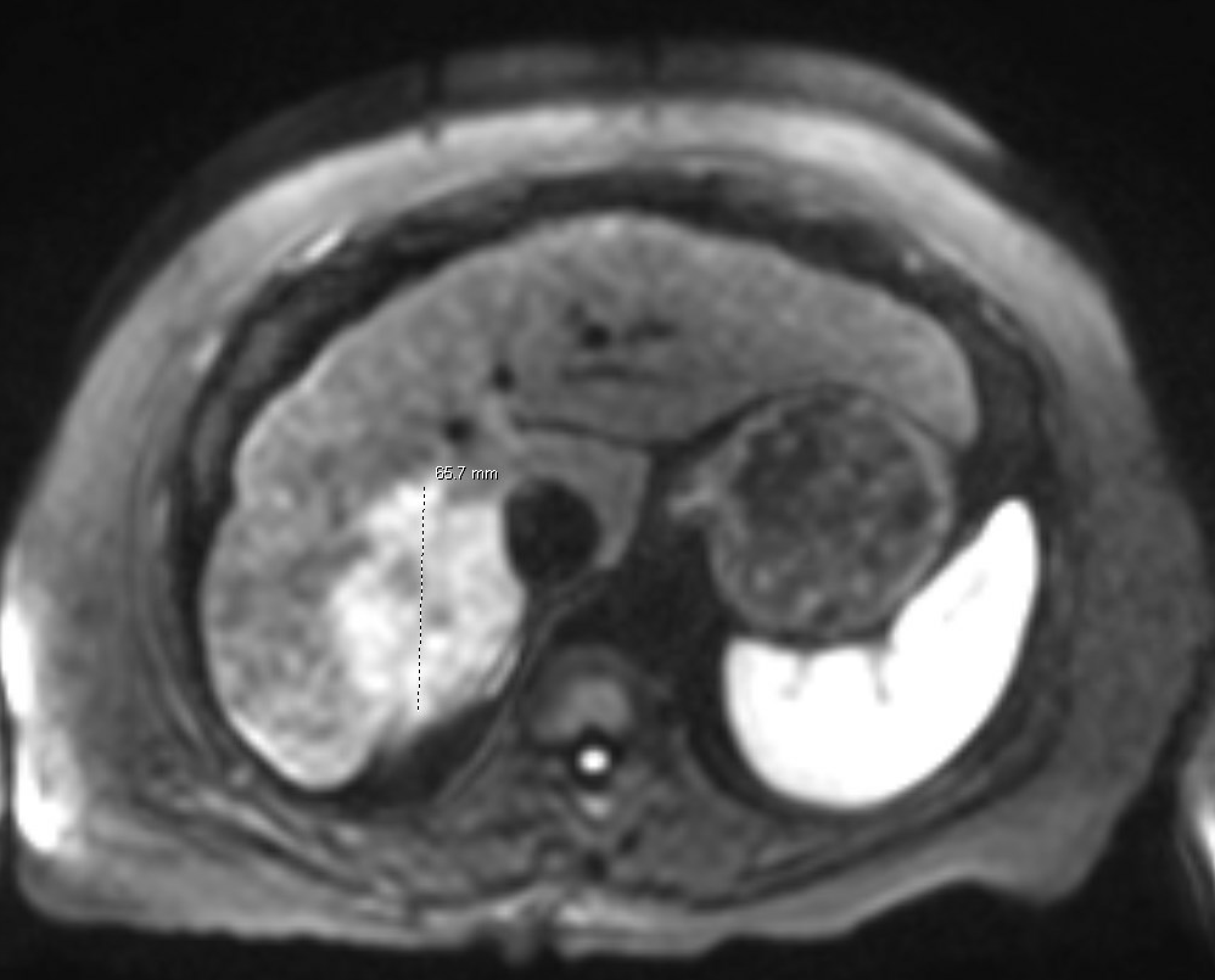
Figure: An MRI of the abdomen showing an approximately 6.5 cm hepatic lesion.
Disclosures: Shiv Patel indicated no relevant financial relationships. Hari Movva indicated no relevant financial relationships. Lucia Soca Gallego indicated no relevant financial relationships. Mahnur Haider indicated no relevant financial relationships. Sreeram Parupudi indicated no relevant financial relationships.
Shiv R. Patel, MD1, Hari Movva, MD2, Lucia Soca Gallego, DO2, Mahnur Haider, MD2, Sreeram Parupudi, MD2. P1741 - When Liver Cancer Reaches the Heart: A Case of Hepatocellular Carcinoma With Rare Right Atrial and Inferior Vena Cava Involvement, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

.jpg "Shiv R. Patel, MD photo")