Shravya R. Ginnaram, MD, Katerina Roma, DO, Omid Sanaei, MD, Marco Olivera-Martinez, MD University of Nebraska Medical Center, Omaha, NE Introduction: Spontaneous hepatic lobe torsion is a rare finding and typically associated with congenital anomalies such as accessory or pedunculated lobes with inadequate ligamentous anchoring. Torsion may lead to vascular outflow obstruction and ischemic hepatitis. Timely recognition and surgical intervention are critical to avoid irreversible liver damage.
Case Description/
Methods: A 76-year-old female with a history of hypertension, hyperlipidemia, and prior morbid obesity (weight loss from 380 lbs to 170 lbs) presented with acute onset nausea, abdominal cramping, and profuse diarrhea. Symptoms progressed to persistent epigastric and upper abdominal pressure radiating to the chest and back. Initial laboratory evaluation revealed marked transaminitis with AST 1252 U/L and ALT 1249 U/L. Otherwise unremarkable total bilirubin 0.7 mg/dL, alkaline phosphatase 37 U/L, and INR 1.2. Alternative workup for acute liver injury including viral hepatitis and autoimmune etiology was unremarkable. Imaging identified torsion of the left hepatic lobe with associated portal and hepatic vein thrombosis and choledocholithiasis. Exploratory laparotomy confirmed axial torsion of an elongated and pedunculated ischemic left hepatic lobe with multiple capsule ruptures and a left lobectomy was performed. Postoperative course was uncomplicated and liver enzymes rapidly normalized. Histopathology showed severe congestion, pericentral hepatocyte necrosis, and organizing intravascular thrombus. Additional benign findings included a sclerosed angioma and von Meyenburg complexes. The resected falciform ligament consisted only of fibrofatty tissue. Discussion: The patient’s elongated and mobile left lobe, narrow pedicle, and absence of supportive ligamentous structures likely predisposed to torsion. Significant prior weight loss may have contributed by reducing visceral fat and weakening hepatic anchoring. While accessory lobes are a known congenital risk factor, this case highlights that acquired anatomic changes can also lead to torsion.
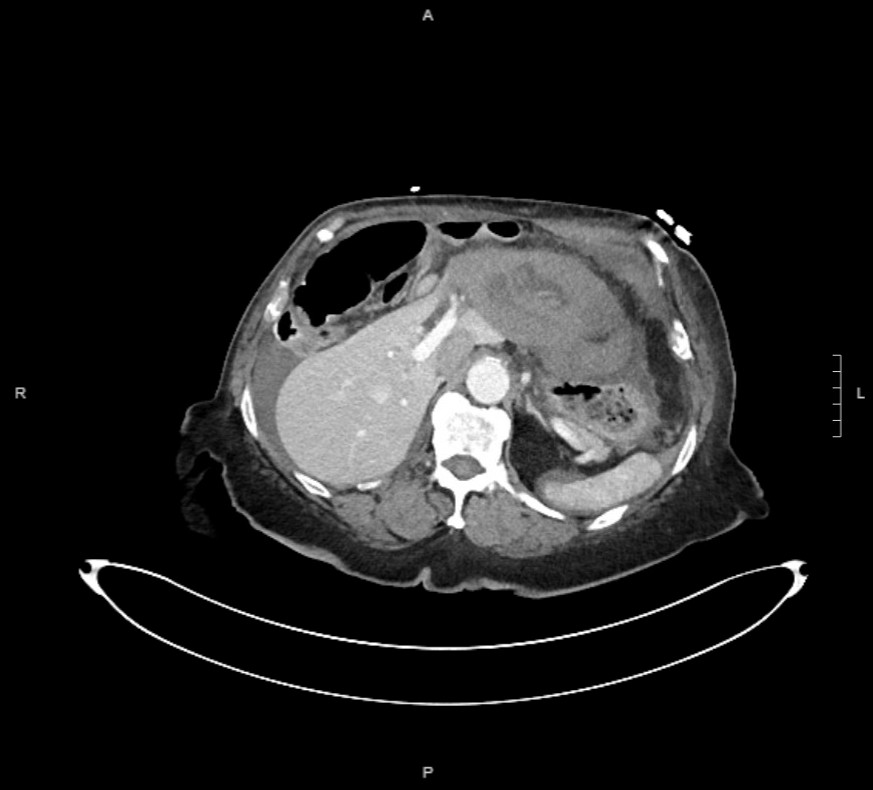
Figure: Axial contrast-enhanced CT abdomen showing engorgement and reduced enhancement of the left lateral segment of the liver. There is absent opacification of the left hepatic vein and decreased enhancement of the left portal vein branches, consistent with segmental vascular compromise due to hepatic lobe torsion.
Disclosures: Shravya Ginnaram indicated no relevant financial relationships. Katerina Roma indicated no relevant financial relationships. Omid Sanaei indicated no relevant financial relationships. Marco Olivera-Martinez indicated no relevant financial relationships.
Shravya R. Ginnaram, MD, Katerina Roma, DO, Omid Sanaei, MD, Marco Olivera-Martinez, MD. P1725 - Spontaneous Left Hepatic Lobe Torsion: A Rare Cause of Ischemic Hepatitis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.