Mahinaz Mohsen, MD1, Ethan Shamsian, MD1, Lyndon Zhu, BA1, Sai Vendidandi, BS1, Rohan Karkra, MBBS1, Michael Bebawy, DO1, Yunseok Namn, MD2 1Rutgers New Jersey Medical School, Newark, NJ; 2Cooperman Barnabas Medical Center, Livingston, NJ Introduction: Antiphospholipid syndrome (APS) is an autoimmune disorder marked by recurrent venous and arterial thromboses due to antiphospholipid antibodies. Catastrophic APS (CAPS) is a rare, rapidly progressive form characterized by widespread small vessel thrombosis and multiorgan failure. Gastrointestinal (GI) involvement is uncommon but typically includes liver complications such as Budd-Chiari syndrome and hepatic infarction due to hepatic vein thrombosis. Other GI manifestations include mesenteric and splenic infarction and gastric ulcers. We present a case of a 32-year-old male with vague abdominal pain, ultimately diagnosed with early CAPS, highlighting the need for awareness of atypical CAPS presentations involving the GI system.
Case Description/
Methods: A 32-year-old male with quadruple-positive APS, rheumatoid arthritis, and Gilbert syndrome presented with facial rash, abdominal pain, and vomiting after switching from warfarin to low molecular weight heparin for elective surgery. Initial labs showed mild transaminitis (AST 39 U/L, ALT 86 U/L), thrombocytopenia (Platelets 133), and INR 1.44. CT abdomen/pelvis showed splenomegaly and gastric distension without evidence of infarction (Figures 1A-C). EGD showed diffuse gastritis and gastric purpura (Figures 2A-C). He developed worsening abdominal pain, fevers, and acute kidney injury. On day 4, imaging showed multiple new hepatic infarcts (Figures 1D-F) and splenic lesions. Repeat labs: AST 383 U/L, ALT 927 U/L, platelets 45. He was diagnosed with CAPS and received steroids, plasmapheresis, and anticoagulation with initial improvement. He was transferred to another institution for further CAPS management. On day 9, severe epigastric pain recurred with new multifocal hepatic and splenic infarcts. He was treated with another steroid course, plasmapheresis, and Rituximab, with significant improvement. He was discharged home on prednisone, atovaquone, pantoprazole, warfarin, and vitamin D. Discussion: This is a rare case of CAPS presenting as non-specific abdominal pain following warfarin discontinuation. While gastrointestinal symptoms are rare in APS, they are more common in CAPS, particularly involving the liver and spleen. However, abdominal pain as a primary symptom is rarely reported, especially in adults. This case underscores the need for high clinical suspicion for hepatic and splenic infarction in APS patients with vague abdominal symptoms, especially with subtherapeutic INR. It supports early and repeat CT or MRI imaging to aid diagnosis.
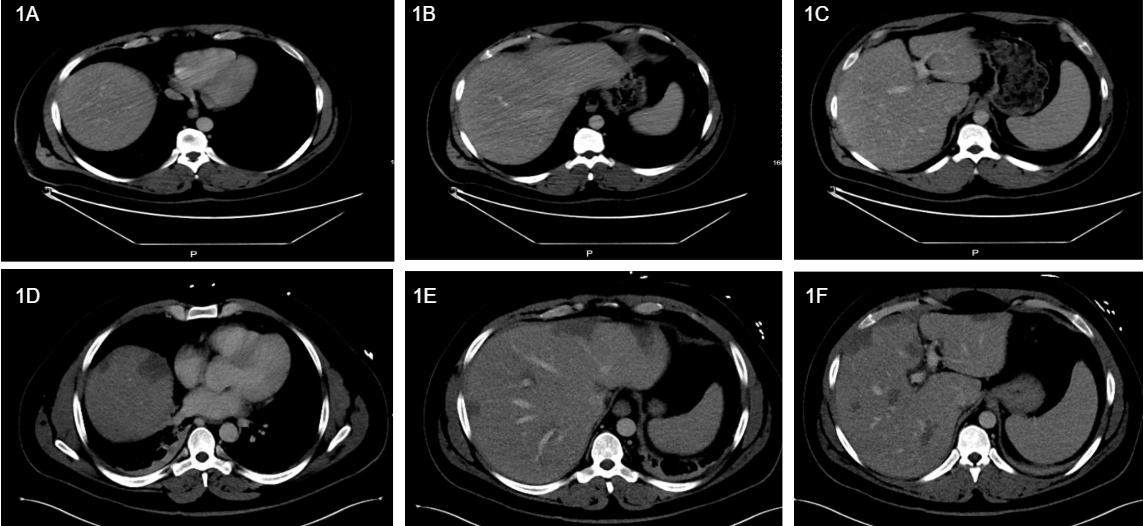
Figure: Figures 1A-C: Initial CT A/P of the liver reveals an enlarged spleen and gastric distention without evidence of infarction. Figures 1D-F: Repeat CT A/P imaging done after APS flare-up, four days after initial presentation. Multiple new hypoattenuating lesions in the liver are visible, consistent with multiple infarcts.
Figure: Figures 2A-2C: Esophagogastroduodenoscopy to work up gastric distension showed diffuse inflammation indicating gastritis in the body and upper body of the stomach (2A, 2B), with scattered gastric purpura in the antrum (2C).
Disclosures: Mahinaz Mohsen indicated no relevant financial relationships. Ethan Shamsian indicated no relevant financial relationships. Lyndon Zhu indicated no relevant financial relationships. Sai Vendidandi indicated no relevant financial relationships. Rohan Karkra indicated no relevant financial relationships. Michael Bebawy indicated no relevant financial relationships. Yunseok Namn indicated no relevant financial relationships.
Mahinaz Mohsen, MD1, Ethan Shamsian, MD1, Lyndon Zhu, BA1, Sai Vendidandi, BS1, Rohan Karkra, MBBS1, Michael Bebawy, DO1, Yunseok Namn, MD2. P1723 - A Case of Catastrophic Antiphospholipid Syndrome Manifesting as Abdominal Pain, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")