Hospital Roosevelt / Gastri-k Guatemala City, San Marcos, Guatemala
Kevin Quijada, 1, Jorge Obando, 2, Isaac Lewin, 3, Marcelino Champet, 4, Yuli Toledo, 5, Bryan Torres, MD6, Abel Sanchez, MD, MSc7 1Gastroenterology & Digestive Endoscopy Unit, Roosevelt Hospital, Guatemala City, Jalapa, Guatemala; 2Gastroenterology & Digestive Endoscopy Unit, Roosevelt Hospital, University of San Carlos of Guatemala, Guatemala City, Chimaltenango, Guatemala; 3Gastroenterology & Digestive Endoscopy Unit, Roosevelt Hospital, Guatemala City, Chimaltenango, Guatemala; 4Gastroenterology & Digestive Endoscopy Unit, Roosevelt Hospital, Guatemala City, Quetzaltenango, Guatemala; 5Gastroenterology an Digestive Endoscopy, Hospital Roosevelt, Guatemala, Guatemala City, Chimaltenango, Guatemala; 6Gastroenterology & Digestive Endoscopy Unit, Roosevelt Hospital, University of San Carlos of Guatemala, Guatemala City, Quetzaltenango, Guatemala; 7Hospital Roosevelt / Gastri-k, Guatemala City, San Marcos, Guatemala Introduction: Drug-induced liver injury (DILI) is an idiosyncratic adverse reaction and a leading cause of acute non-infectious liver damage. It presents as liver biochemical abnormalities triggered by medications, herbs, or supplements. Incidence is 10–15 per 100,000 individuals; antibiotics account for 50% of cases. Amoxicillin-clavulanate has an estimated incidence of 1 in 7,000, especially in males >55. We report a case of jaundice after amoxicillin-clavulanate exposure in a 76-year-old man
Case Description/
Methods: A 76-year-old male with controlled type 2 diabetes developed jaundice after a 10-day course of amoxicillin-clavulanate for pharyngeal erythema due to foreign body trauma. Labs: total bilirubin 19.2 mg/dL (direct 16.9), ALP 171, GGT 183, AST 76, ALT 140, INR 1.58. Viral and autoimmune causes were excluded. R-factor: 4.9 (mixed injury); RUCAM: 6 (probable DILI). Imaging showed hepatomegaly and gallbladder wall thickening. Liver biopsy: cholestatic hepatitis with periportal inflammation. Withdrawal of the drug led to clinical and biochemical resolution Discussion: DILI, often due to antibiotics, is a major cause of acute liver injury. Amoxicillin-clavulanate frequently causes cholestatic or mixed patterns, with bilirubin and ALP elevation. Risk factors: male sex, age >55, prior exposure, HLA-DRB1*1501. Clavulanate likely triggers immune-mediated damage. Management is supportive and based on drug cessation. This case highlights the importance of early recognition of DILI and reinforces pharmacovigilance amid widespread antibiotic use
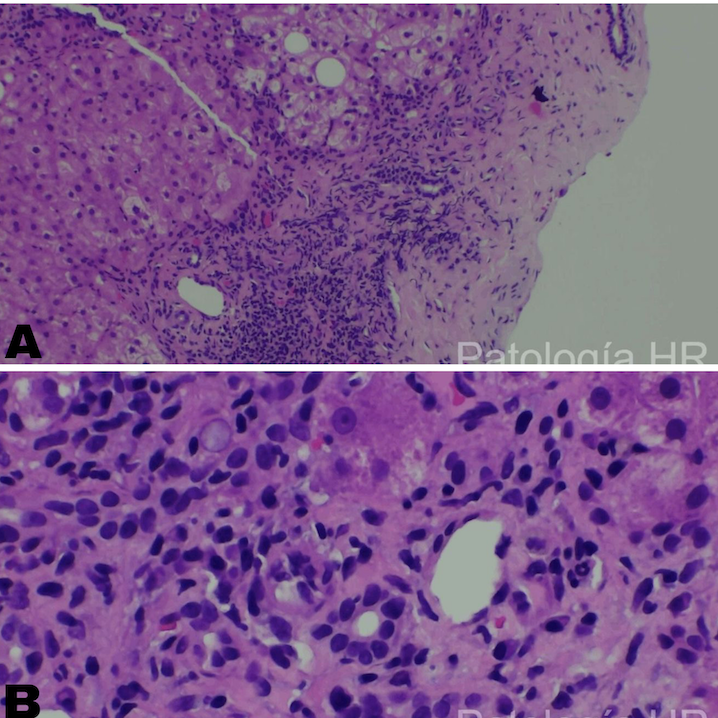
Figure: Figure1. Cholestatic hepatitis: Hepatocytes exhibiting cytoplasmic bile pigment and a moderate chronic inflammatory infiltrate at the interface and periportal areas, with sparse neutrophils (A). Bile duct proliferation is observed, accompanied by areas of fibrosis (B).
Disclosures: Kevin Quijada indicated no relevant financial relationships. Jorge Obando indicated no relevant financial relationships. Isaac Lewin indicated no relevant financial relationships. Marcelino Champet indicated no relevant financial relationships. Yuli Toledo indicated no relevant financial relationships. Bryan Torres indicated no relevant financial relationships. Abel Sanchez indicated no relevant financial relationships.
Kevin Quijada, 1, Jorge Obando, 2, Isaac Lewin, 3, Marcelino Champet, 4, Yuli Toledo, 5, Bryan Torres, MD6, Abel Sanchez, MD, MSc7. P1695 - Hidden Hepatotoxicity: Amoxicillin-Clavulanate-Induced Liver Injury in a Diabetic Patient, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")