P1614 - Rising Rates of Hepatocellular Carcinoma Mortality in the United States From 1999 to 2024: A Comprehensive 25-Year Analysis by Demographic, Regional, and Urbanization Factors
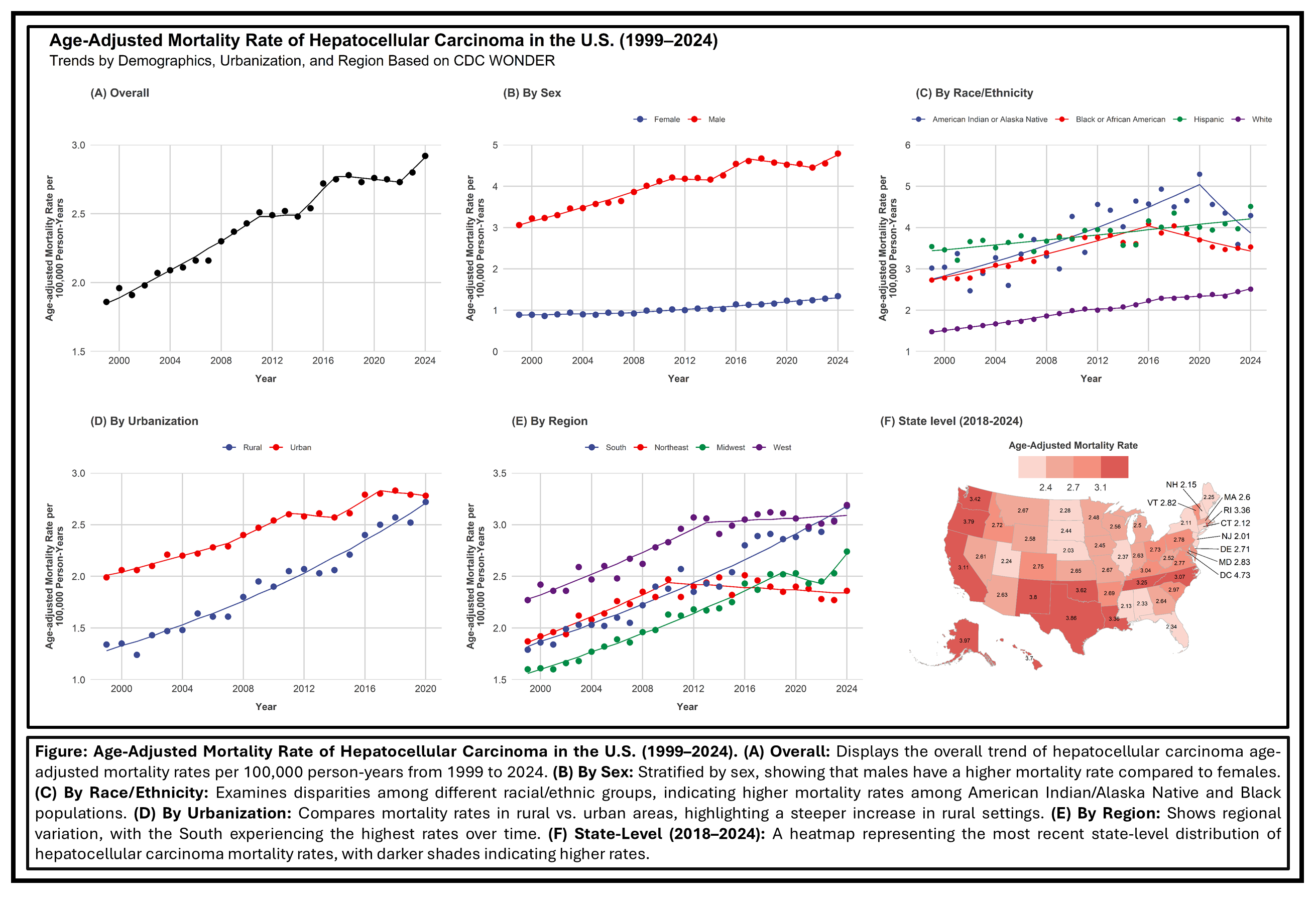
Mohamed A. B. Elnaggar, MD1, Ibrahim Hassan, MBBCh2, Hatem Eltaly, MD3, Ayah Obeid, MD4, Mohamed Abd El Aziz, MD5, Kamran Qureshi, MD6 1Hartford Healthcare, Hartford, CT; 2Faculty of Medicine, Suez Canal University, Ismailia, Al Isma'iliyah, Egypt; 3Cleveland Clinic Foundation, Cleveland, OH; 4St. Luke's University Health Network, Bethlehem, PA; 5Deaconess health system, Henderson, KY; 6Saint Louis University School of Medicine, Saint Louis, MO Introduction: Hepatocellular carcinoma (HCC) mortality has been rising in the United States, yet contemporary data on how these trends vary by sex, race/ethnicity, region, and urbanization are limited. We aimed to characterize changes in age-adjusted mortality rates (AAMRs) of HCC from 1999 to 2024 using nationwide surveillance data Methods: We obtained data on HCC deaths (n=234,528) from the Centers for Disease Control and Prevention Wide-ranging Online Data for Epidemiologic Research (DC WONDER) database for the period1999–2024 with by its ICD-10 code (C22.0). AAMRs were calculated per 100,000 population, age-adjusted to the 2000 U.S. standard population. Joinpoint regression analysis was used to identify significant trend segment changes and estimate segment-specific annual percent changes (APCs) and overall average annual percent changes (AAPCs). Results: Mortality rates due to HCC have increased from 1.86 (95% CI: 1.80 to 1.91) in 1999 to 2.92 (2.87 to 2.97) in 2024 (AAPC: 1.83%, 95% CI: 1.69 to 1.97). Throughout the period, males consistently exhibited higher mortality rates than females, with rates of 4.79 versus 1.34 in 2024, respectively. Although white patients maintained the lowest AAMR over the 25 years, they experienced the most rapid increase (AAPC: 2.18%, 95% CI: 2.04 to 2.3) among racial/ethnic groups.
Regionally, the South exhibited the highest 2024 AAMR (3.18), with an AAPC of 2.25%. The AAMR gap between rural and urban areas is closing, and rural areas had a more pronounced increase (1.34 to 2.72, APC: 3.63%) compared to the urban areas (AAMR 1.99 to 2.78, AAPC: 1.56%).
Even though some subpopulations have experienced reversals, deceleration, or stabilization in trends, the overall mortality from HCC continues to increase. Discussion: HCC mortality continues to rise across the United States, with marked disparities by sex, race/ethnicity, region, and urbanization status. These findings underscore the urgent need for targeted prevention strategies, improved screening, and equitable access to care, particularly for high-risk populations and rural communities, to mitigate the growing burden of HCC.
Figure: Age adjusted Mortality Rate of HCC in the U.S. (1999-2024)
Disclosures: Mohamed A. Elnaggar indicated no relevant financial relationships. Ibrahim Hassan indicated no relevant financial relationships. Hatem Eltaly indicated no relevant financial relationships. Ayah Obeid indicated no relevant financial relationships. Mohamed Abd El Aziz indicated no relevant financial relationships. Kamran Qureshi: Gilead Sciences – Speakers Bureau. Intercept Pharmaceuticals – Speakers Bureau. Madrigal Pharmaceuticals – Speakers Bureau. Phathom Pharmaceuticals – Speakers Bureau. Salix Pharmaceuticals – Speakers Bureau.
Mohamed A. B. Elnaggar, MD1, Ibrahim Hassan, MBBCh2, Hatem Eltaly, MD3, Ayah Obeid, MD4, Mohamed Abd El Aziz, MD5, Kamran Qureshi, MD6. P1614 - Rising Rates of Hepatocellular Carcinoma Mortality in the United States From 1999 to 2024: A Comprehensive 25-Year Analysis by Demographic, Regional, and Urbanization Factors, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.