Stony Brook University Hospital Port Jefferson Station, NY
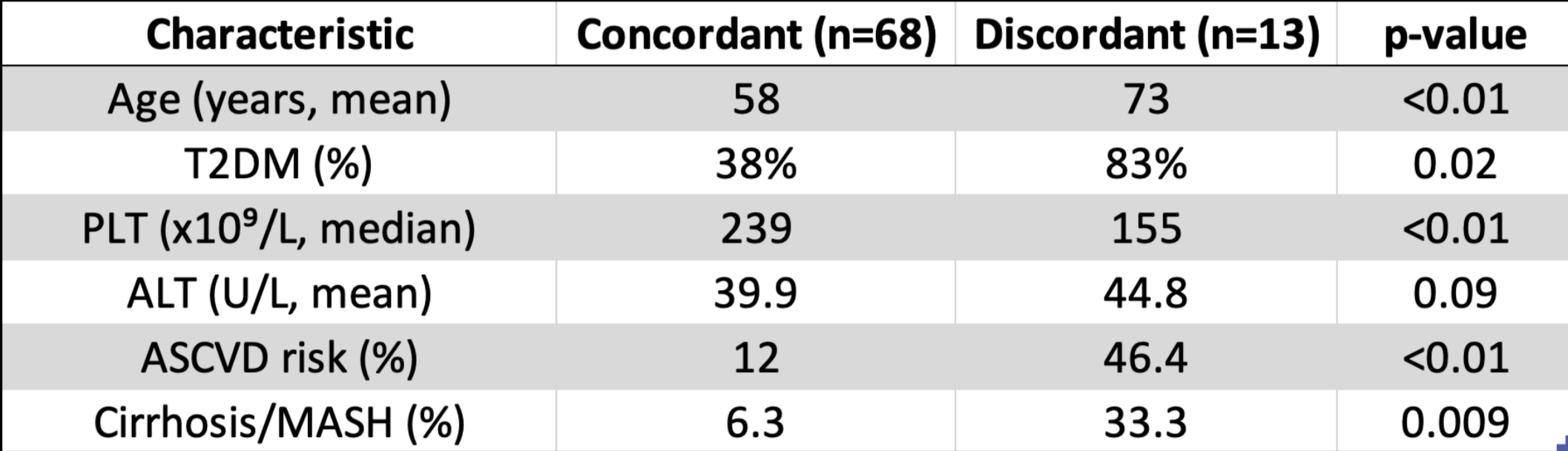
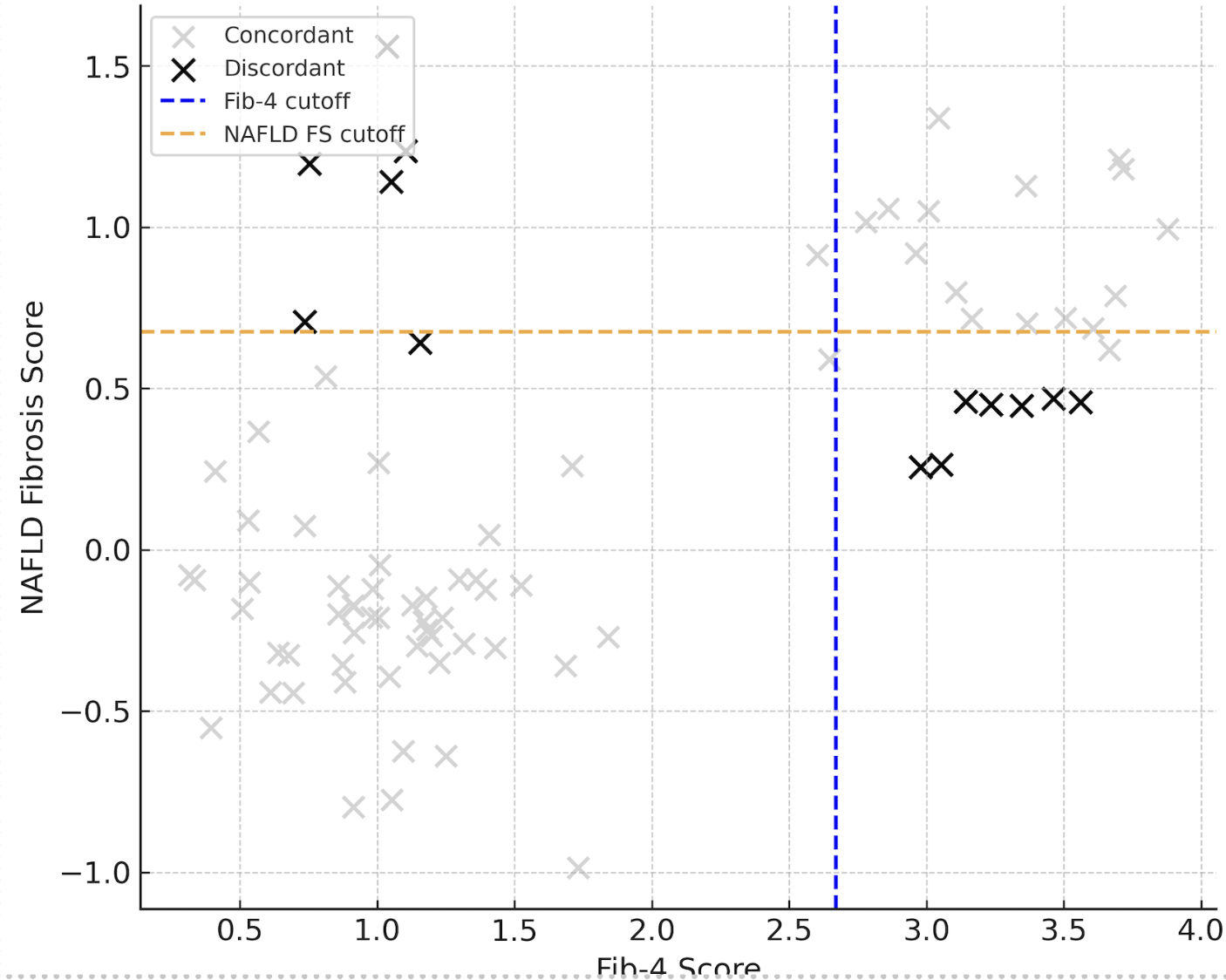
Jacky Reny, MD1, Jordan Barnett-Kradjian, DO2, Kaustav Patra, MD1, Pallavi Kawatra, BS3, Lisa Fisher, MD4 1Stony Brook University Hospital, Port Jefferson Station, NY; 2Stony Brook Medicine, Stony Brook, NY; 3Philadelphia College of Osteopathic Medicine, Philadelphia, PA; 4Stony Brook University Hospital, Northport, NY Introduction: Noninvasive fibrosis scores, including Fib-4 and the NAFLD fibrosis score, are widely recommended for risk stratification in patients with MASLD. However, the concordance between these two scores—and the clinical implications of discordance—remain poorly understood, particularly in cohorts with substantial heterogeneity. Understanding the prevalence, predictors, and outcomes of discordant results may inform more nuanced clinical decision-making, referral strategies, and patient management. We aimed to determine the frequency and clinical significance of discordance between Fib-4 and NAFLD fibrosis score in a MASLD cohort. Methods: We performed a retrospective analysis of 80 adults with MASLD seen at a veteran's affairs hospital. Discordance was defined as placement in different risk categories by Fib-4 and NAFLD fibrosis score using established cutoffs (Fib-4 >2.67; NAFLD FS >0.676). Multiple demographic and clinical features were compared between discordant and concordant groups. Multivariable logistic regression identified predictors of discordance. Clinical outcomes—including the prevalence of cirrhosis and MASH—were compared between groups. Results: Of 80 patients, 13 (15.8%) demonstrated discordance between Fib-4 and NAFLD fibrosis score. Discordant patients were significantly older (mean age 73 vs. 58 years), more likely to have diabetes (83% vs. 38%), had lower platelet counts (median 155 vs. 239 x10⁹/L), higher ALT (mean 44.8 vs. 39.9 U/L), and much higher ASCVD 10-year risk (46.4% vs. 12.0%) compared to concordant patients. Older age (OR per year: 1.13, 95% CI 1.04–1.23, p = 0.003) and T2DM (OR: 4.5, 95% CI 1.2–16.7, p = 0.024) were independently associated with discordance. The prevalence of cirrhosis or MASH higher in discordant patients (33.3%) compared to concordant patients (6.3%) (p = 0.009). Discussion: Discordance between Fib-4 and NAFLD fibrosis score occurs in approximately 16% of MASLD patients and is strongly associated with older age, diabetes, lower platelet counts, and higher cardiovascular risk. Discordant patients experienced a greater than fivefold increased prevalence of cirrhosis or MASH compared to those with concordant scores, highlighting the clinical importance of recognizing and managing discordant findings. These results support the need for cautious interpretation of noninvasive fibrosis scores in high-risk populations. Prospective validation and investigation of optimal management strategies for discordant patients are warranted.
Figure: Clinical Features and Outcomes by Concordance Status
Figure: Discordance Between Fib-4 and NAFLD Fibrosis Score
Disclosures: Jacky Reny indicated no relevant financial relationships. Jordan Barnett-Kradjian indicated no relevant financial relationships. Kaustav Patra indicated no relevant financial relationships. Pallavi Kawatra indicated no relevant financial relationships. Lisa Fisher indicated no relevant financial relationships.
Jacky Reny, MD1, Jordan Barnett-Kradjian, DO2, Kaustav Patra, MD1, Pallavi Kawatra, BS3, Lisa Fisher, MD4. P1592 - Discordance Between Noninvasive Fibrosis Scores in MASLD: Clinical Predictors and Outcomes in a Veteran Population, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")