Preeyati Chopra, MBBS1, Khushboo Gala, MD2, Mayank Goyal, MBBS2, Ashwariya Ohri, MBBS3, Mahin Bhatt, MBBS2, Ryan Law, DO2 1Mayo Clinic, Hartford, CT; 2Mayo Clinic, Rochester, MN; 3Mayo Clinic, Indianapolis, IN Introduction: Peptic ulcer disease (PUD) refractory to standard high dose proton pump inhibitor (PPI) therapy raises concerns for patient non-compliance, rapid CYP metabolizers or an atypical underlying etiology including malignancy or Crohn’s disease. We describe a patient with a refractory gastric ulcer, found to have diffuse large–cell lymphoma (DLBCL).
Case Description/
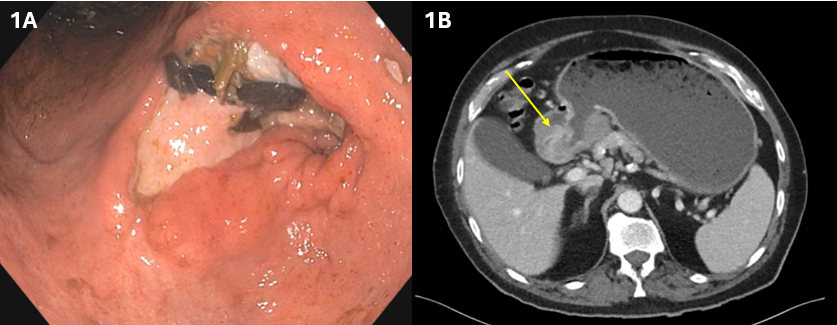
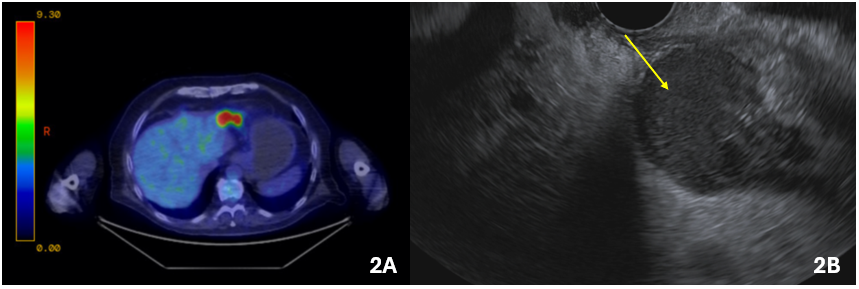
Methods: A 72-year-old man presented with multiple episodes of gastrointestinal bleeding over 6 months, attributed to PUD despite the use of high-dose PPIs. He was found to have rapid metabolism of CYP2C19 and hence started on vonoprazan. Despite this, he continued to have melena and abdominal pain. Laboratory tests noted a hemoglobin drop from 16.8 to 10.5 within a month. He underwent endoscopy, that showed a large, non-bleeding cratered gastric ulcer with a clean ulcer base (Forrest Class III) in the antrum (Figure 1A) with benign-appearing, intrinsic severe stenosis immediately distal to the ulcer. Prior endoscopic biopsies were negative. Further workup for the etiology of this ulcer was pursued. CT imaging revealedgastric distension,irregular thickening of the peripyloric region (Figure 1B) with mildly prominent adjacent lymph nodes. Positron Emission Tomography-CT showed abnormal 18‐fluorodeoxyglucose uptake within the gastric antrum with a maximum standardized uptake value of 26.7 (Figure 2A). EUS revealed a hypoechoic intramural (subepithelial) lesion in the antrum appearing to originate from muscularis propria (layer 4), underlying the area of ulceration (Figure 2B). Fine needle biopsies were obtained, and pathological findings revealed diffuse proliferation of large atypical lymphoid cells. Immunohistochemical staining was positive for CD10, CD20, BCL6, and MYC. The patient was diagnosed with DLBCL, Not Otherwise Specified (Germinal Center B-cell phenotype) and has started treatment. Discussion: This case demonstrates the importance of evaluating for underlying etiologies in cases with refractory or atypical presentations PUD.

 photo")