Texas Tech University Health Sciences Center El Paso, TX
Bansi Sutariya, MD, Gerardo R. Gutierrez-Sierra, MD, Abirami Rajendiran, MD, Deipthan Prabakar, MD, Azucena Del Real, MD Texas Tech University Health Sciences Center, El Paso, TX Introduction: Emphysematous gastritis is a rare, life-threatening form of gastritis marked by gas within the gastric wall due to invasion by gas-forming organisms. While typically seen in patients with comorbidities such as diabetes mellitus, immunosuppression, or alcohol use disorder, it can also occur in younger patients with more subtle risk factors. The condition presents with nonspecific gastrointestinal symptoms like abdominal pain, nausea, and vomiting, often delaying diagnosis. Early recognition is critical, as it can progress to gastric necrosis, sepsis, and death if untreated. Computed tomography remains the gold standard for diagnosis, helping differentiate it from gastric emphysema—a benign, noninfectious condition with a favorable prognosis and mostly conservative treatment.
Case Description/
Methods: We present two distinct cases of emphysematous gastritis successfully managed without surgical intervention. The first involves a 24-year-old previously healthy male with a significant history of chronic alcohol use, presenting with acute epigastric pain and non-bilious vomiting. CT showed intramural gastric gas without signs of perforation He was managed conservatively with bowel rest, IV fluids, nasogastric decompression, IV pantoprazole, and empiric antibiotics (Piperacillin/tazobactam). Surgical intervention was not required, he improved within 72 hours and was discharged on oral antibiotics. The second case involves a 78-year-old male with alcoholic cirrhosis and recent NSAID use, presenting with epigastric pain, vomiting, and diarrhea. CT revealed gas in the gastric wall and portal venous system. Despite his comorbidities and concurrent acute kidney injury, he remained stable. He was treated with IV fluids, bowel rest, and pantoprazole. Endoscopy showed diffuse inflammation without necrosis or perforation, and he was discharged on oral pantoprazole with instructions to avoid NSAIDs. Discussion: These cases illustrate that emphysematous gastritis may present across a broad clinical spectrum—from young adults with isolated behavioral risk factors to elderly patients with cirrhosis and NSAID exposure. Conservative management with close monitoring can lead to excellent outcomes in the absence of systemic toxicity or surgical indications. Timely diagnosis, guided by clinical suspicion and confirmatory imaging, along with individualized treatment plans, are essential for optimal patient care in this rare but potentially fatal condition.
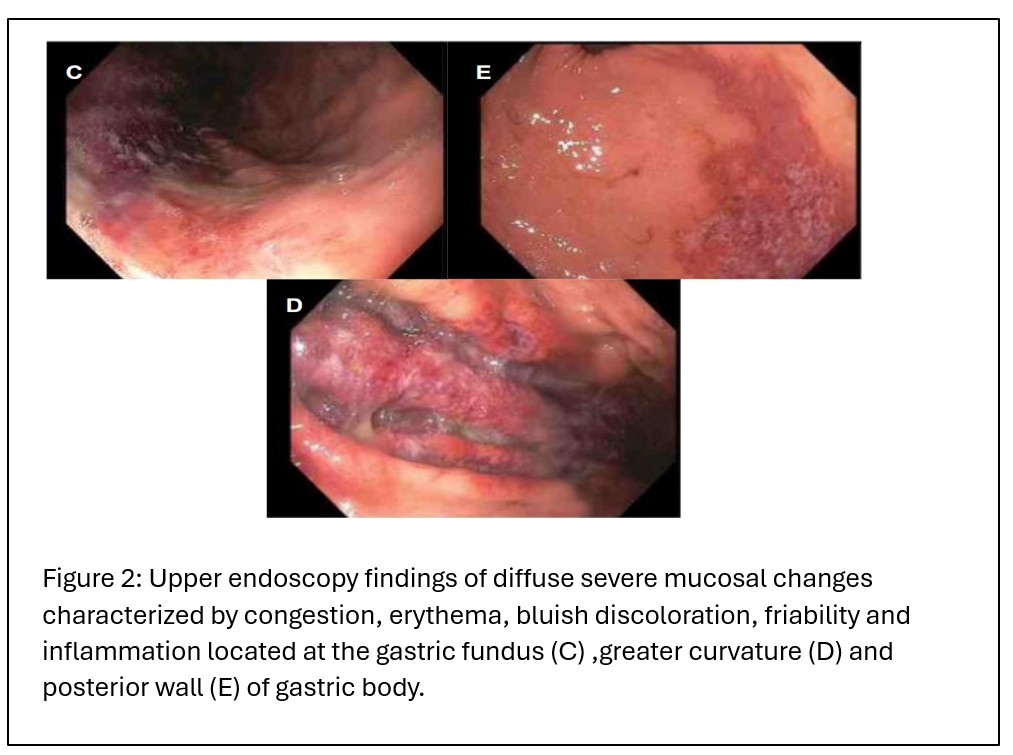
Figure: Figure 1: Upper endoscopy findings of diffuse severe mucosal changes characterized by congestion, erythema, bluish discoloration, friability and inflammation located at the gastric fundus (C) ,greater curvature (D) and posterior wall (E) of gastric body
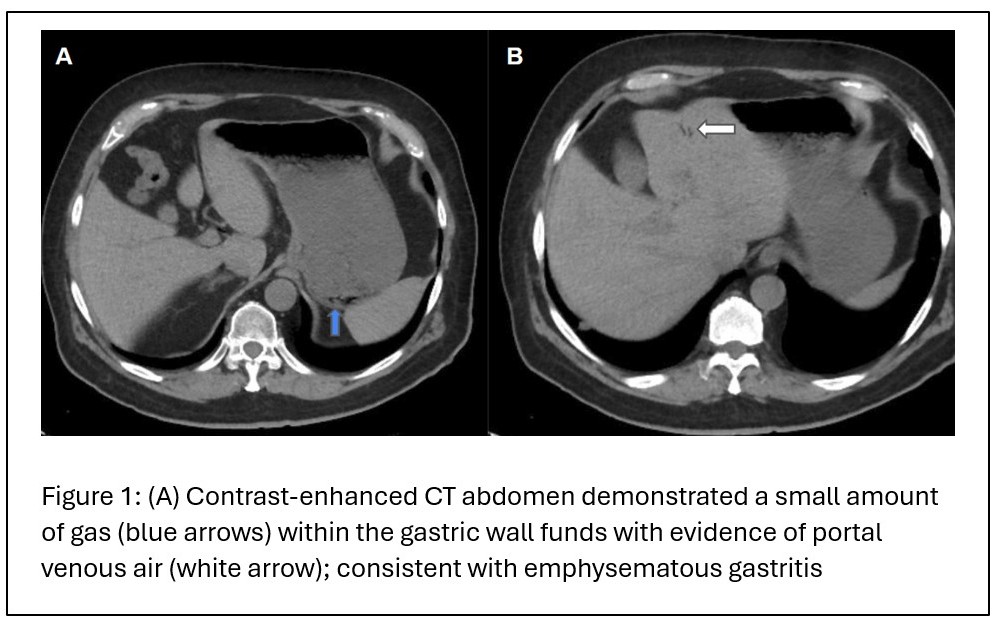
Figure: Figure 2: (A) Contrast-enhanced CT abdomen demonstrated a small amount of gas (blue arrows) within the gastric wall fundus with evidence of portal venous air (white arrow); consistent with emphysematous gastritis.
Disclosures: Bansi Sutariya indicated no relevant financial relationships. Gerardo Gutierrez-Sierra indicated no relevant financial relationships. Abirami Rajendiran indicated no relevant financial relationships. Deipthan Prabakar indicated no relevant financial relationships. Azucena Del Real indicated no relevant financial relationships.
Bansi Sutariya, MD, Gerardo R. Gutierrez-Sierra, MD, Abirami Rajendiran, MD, Deipthan Prabakar, MD, Azucena Del Real, MD. P1353 - Conservative Management of Emphysematous Gastritis in Diverse Clinical Contexts: A Case Series, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.