Brian Holliday, MD1, Rachel Patel, DO2, Timothy Graziano, DO1, Michael Goldner, DO1 1Lehigh Valley Health Network, Allentown, PA; 2Lehigh Valley Health Network, Coopersburg, PA Introduction: Jamaica attracts over 1.2 million tourists annually, offering vibrant culture and natural beauty. However, travel to the region poses risks of acquiring infections. The CDC’s Yellow Book highlights potential hazards including enteric infections (e.g., traveler’s diarrhea), waterborne illnesses (e.g., leptospirosis), and vector-borne diseases (e.g., chikungunya, dengue, Zika, malaria). Here, we present an interesting case of diarrhea secondary to multiple endemic culprits.
Case Description/
Methods: A 46-year-old woman with a history of cutaneous sarcoidosis and Raynaud's phenomenon presented with a two-week history of generalized weakness, myalgias, arthralgias, abdominal pain, nausea, vomiting, diarrhea, headache, and fever. She had recently returned from Jamaica, where she drank tap water, swam in the ocean with an open toe wound, ate local cuisine, and was bitten by insects, including mosquitoes. On examination, she had fever, tachycardia, bilateral conjunctival injection, tender cervical lymphadenopathy, and mild lower extremity edema. Labs noted acute kidney injury (creatinine: 3.7 mg/dL; baseline: ~0.9 mg/dL), elevated inflammatory markers (CRP: 198.8 mg/L, ESR: 45 mm/hr), weakly positive ANA (1:80), and hepatosplenomegaly with small bilateral pleural effusions on CT imaging.
She was empirically treated with doxycycline and ceftriaxone, alongside supportive care. Given her autoimmune history Rheumatology was consulted and completed a workup to rule out progression of her Sarcoidosis or other autoimmune cause of her fever. A stool panel revealed Norovirus and enteropathogenic E. coli (EPEC) so antibiotics were discontinued. Despite only partially improved symptoms and multiple pending lab tests, she opted for discharge due to personal obligations. Subsequent testing revealed she was also positive for Leptospirosis and Chikungunya. Doxycycline was prescribed for Leptospirosis. Discussion: This case illustrates an uncommon scenario of multiple concurrent infections, highlighting diagnostic challenges and clinical complexity. Early stool panel results addressed gastrointestinal symptoms but failed to explain systemic features such as conjunctival injection, tender lymphadenopathy, and musculoskeletal pain. The delayed identification of leptospirosis and chikungunya underscores the importance of vigilance when managing travel-related illnesses, maintaining suspicion for simultaneous processes, and critical interpretation of test results, even after one pathogen is identified.
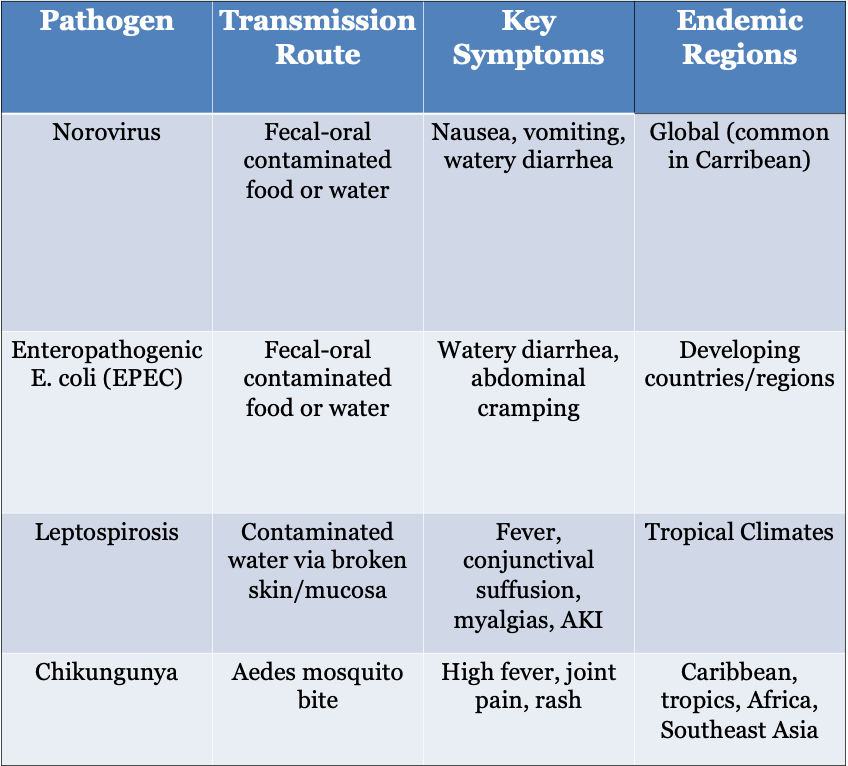
Figure: Table: Summary of potential infectious etiologies considered in the differential diagnosis for a patient presenting with fever, diarrhea, and systemic symptoms following recent travel. The patient’s clinical presentation prompted evaluation for multiple pathogens endemic to tropical and developing regions, including Norovirus, Enteropathogenic E. coli (EPEC), Leptospirosis, and Chikungunya, each with overlapping but distinct transmission routes and symptom profiles.
Disclosures: Brian Holliday indicated no relevant financial relationships. Rachel Patel indicated no relevant financial relationships. Timothy Graziano indicated no relevant financial relationships. Michael Goldner indicated no relevant financial relationships.
Brian Holliday, MD1, Rachel Patel, DO2, Timothy Graziano, DO1, Michael Goldner, DO1. P1341 - Tropical Travels Turned Turbulent: A Case of Multi-Infectious Diarrhea, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

.jpg "Rachel Patel, DO photo")