Wesley Chow, MD1, Rohit Khanna, DO2, Joy-Marie Hermes, MD2, Olivia Lanser, MD2, Ali Fakhreddine, MD3, Gordon Liss, MD4, David Redfield, MD5, Amy Lightner, MD5, Gauree Konijeti, MD, MPH, FACG6 1Scripps Mercy Hospital, San Diego, CA; 2Scripps Green Hospital, La Jolla, CA; 3Scripps Green Hospital, San Diego, CA; 4Scripps Clinic, Oceanside, CA; 5Scripps Clinic, La Jolla, CA; 6Scripps Clinic Medical Group, La Jolla, CA Introduction: Intestinal tuberculosis (TB) is rare in the U.S. and is a diagnostic challenge, mimicking infection and inflammatory bowel disease. Symptoms are nonspecific and complications include intestinal ulcers, strictures, fistulas, ascites or perforation. We present a case of serologic negative intestinal TB mimicking Crohn’s disease.
Case Description/
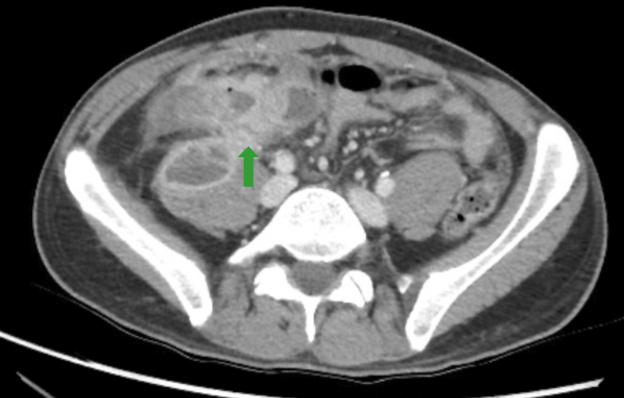
Methods: A 32-year-old Indian born man presented to clinic for 24 hours of generalized abdominal pain, nausea, and vomiting. Labs revealed WBC 14.4K, ESR 21 and CRP 15.1. A CT abdomen and pelvis (CT) noted ascending colitis and mesenteric lymphadenopathy. Infectious workup was negative. Colonoscopy noted mild right-sided colitis without granulomas. His symptoms spontaneously resolved.
His symptoms recurred 18 months later in India. CT showed terminal ileitis and right-sided colitis with pericolic fat stranding. Colonoscopy noted cobblestoning in the terminal ileum and right colon with ulcerations in transverse colon. Biopsies noted chronic active colitis negative for acid-fast bacilli (AFB). He was started on budesonide in India.
One month after returning to the U.S., he presented with worsening abdominal symptoms and weight loss while on budesonide. Labs showed WBC 15K, CRP 147, and fecal calprotectin 2510. CT revealed cecal and ascending colitis with pelvic phlegmon. Infectious workup, including QuantiFERON-TB, was negative. He improved on antibiotics and steroid taper then started risankizumab (RIZ) for presumed ileocolonic Crohn’s disease.
Three months later, he presented with fevers and abdominal pain. CT showed ileitis, right-sided peritonitis and colitis with fistula extension to a 7 cm psoas abscess. Despite initial improvement with percutaneous drainage and antibiotics, he developed loculated pelvic fluid. Laparoscopic diverting ileostomy, without bowel resection, revealed thickened peritoneum with multiple small white tubercles, peritoneal fluid, and colonic omental adhesions. Ascitic fluid returned AFB+, confirming intestinal TB. RIZ was discontinued, and he started TB regimen of rifampin, isoniazid, pyrazinamide and ethambutol (RIPE) with resolution of symptoms. Interval CT, after 2 months of RIPE, was unremarkable. Discussion: Intestinal TB is a known mimicker of Crohn’s disease. Despite negative QuantiFERON and no TB history, he emigrated from an endemic region. This case highlights the importance of maintaining a high index of suspicion in at-risk patients and the need for interdisciplinary care in complex, atypical presentations.


 photo")