Department of Medicine and Department of Epidemiology and Biostatistics, Western University London, ON, Canada
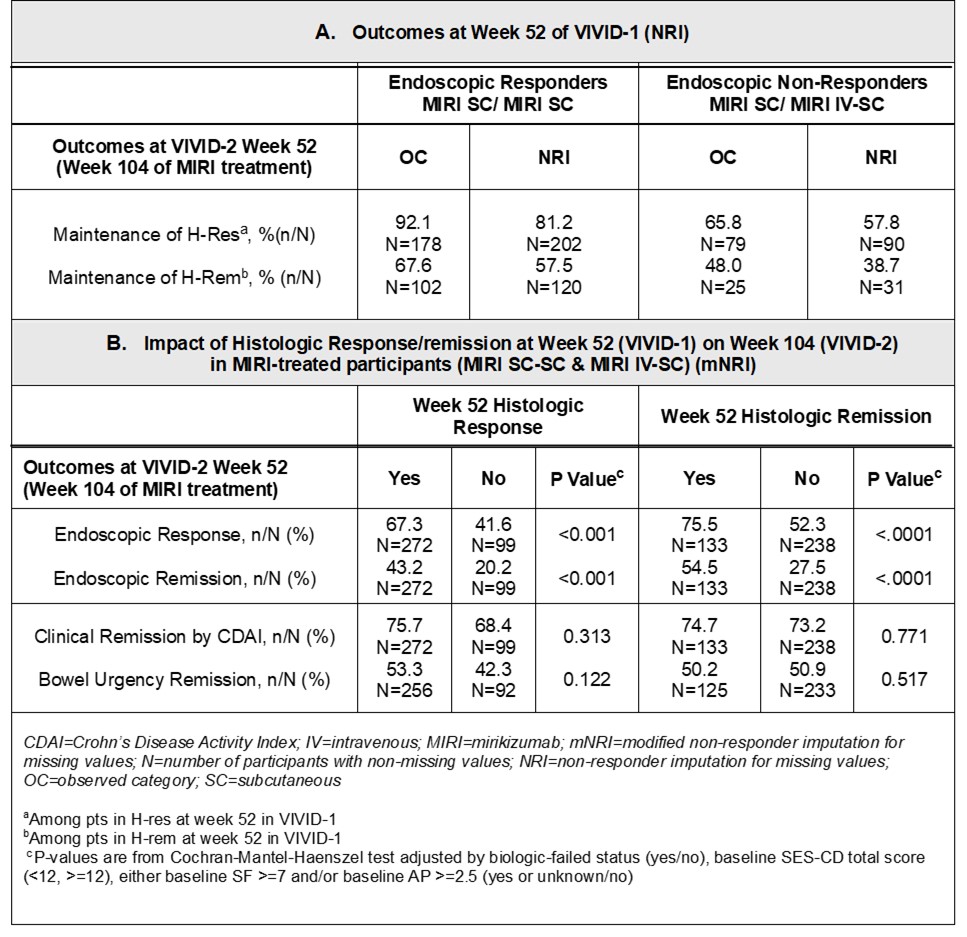
Walter Reinisch, MD, PhD1, Vipul Jairath, MBChB, DPhil, MRCP2, Marijana Protic, 3, Gert De Hertogh, 4, Noam Harpaz, 5, Tadakazu Hisamatsu, MD, PhD6, Geert R. D’Haens, MD, PhD7, Rish Pai, 8, Nathan Morris, 3, Rebecca Hozak, 3, Guanglei Yu, PhD9, Frederick Durand, 3, Fernando Magro, MD, PhD10 1Medical University of Vienna, Department of Internal Medicine III, Division of Gastroenterology and Hepatology, Spitalgasse, Wien, Austria; 2Department of Medicine and Department of Epidemiology and Biostatistics, Western University, London, ON, Canada; 3Eli Lilly and Company, Indianapolis, IN; 4Faculty of Medicine, KU, Leuven, Leuven, Brabant Wallon, Belgium; 5Icahn School of Medicine at Mount Sinai, New York, NY; 6Department of Gastroenterology and Hepatology, Kyorin University School of Medicine, Tokyo, Tokyo, Japan; 7Department of Gastroenterology, Amsterdam University Medical Center, Amsterdam, Noord-Holland, Netherlands; 8Mayo Clinic, Scottsdale, AZ; 9Eli Lilly and Company, Indianapolis, Indiana, USA, Indianapolis, IN; 10University of Porto, Porto, Porto, Portugal Introduction: VIVID-1 evaluated systematically obtained biopsies from 5 intestinal segments demonstrating that histologic (histo) readouts were impacted upon treatment with mirikizumab (MIRI). Methods: VIVID-2, the long-term extension study of VIVID-1, examines histo and combined endoscopic(endo)-histo endpoints at Week(W)104. These data are presented, as is the impact of 1-year(yr) histo response (H-res) and histo remission (H-rem) on endoscopic and clinical outcomes after 2 yrs of MIRI treatment. In VIVID-1, the MIRI group received induction with 900 mg intravenously (IV) at W0, 4, and 8, then 300 mg subcutaneously (SC) every 4W. W52 patients (pts) in endo response (E-res; ≥50% reduction from baseline in Simple Endoscopic Score for CD) continued the same MIRI SC dosing in VIVID-2. Endo non-responders received reinduction with MIRI IV at the start of VIVID-2 followed by SC dosing (IV-SC) as described. Two specimens from each of 5 intestinal segments (1 ileal, 4 colonic) were obtained from the edge of ulcers, or the most inflamed mucosa from randomized pts at screening, W12, W52 (VIVID-1), and W104 (W52 of VIVID-2). H-res: absence of epithelial neutrophils and epithelial damage, erosions, and ulceration or ≥50% decrease in either the active Robarts Histopathology Index or the active Global Histology Activity Score. H-rem: absence of mucosal neutrophils, no epithelial damage, and no erosions and ulcers. The criteria for H-res and H-rem had to be met in all 5 segments. Results: Among pts in E-res at W52 of VIVID-1: 81.2% maintained H-res and 57.5% maintained H-rem after an additional 52 weeks of MIRI SC treatment (Table 1A), 70.8% maintained combined endo-histo response. Interestingly, 25.6% pts who were in H-Res, but not in E-res at W52 of VIVID-1 maintained H-res and gained E-res during the 2nd year of MIRI treatment (IV-SC). In the overall MIRI-treated population (SC-SC and IV-SC), both H-res and H-rem were significantly associated with E-res (p< 0.001) and endo-remission (p< 0.001) at W104 while associations with Crohn’s Disease Activity Index remission (p=0.313 and p=0.771, respectively) and bowel urgency remission (p=0.122 and p=0.517, respectively) were not identified (Table 1B). Discussion: In VIVID-2, achievement of histologic response and remission after 1 yr of miri treatment was strongly associated with longer term endoscopic outcomes. High rates of histologic and combined endo-histo endpoints were maintained after 2 yrs of treatment.
Figure: Week(W) 52 Outcomes and the Impact of Histologic Response/Remission at W52 on W104 in the Overall MIRI-treated Patients