Division of Gastroenterology, Hepatology, and Endoscopy, Brigham and Women’s Hospital, Harvard Medical School Boston, MA
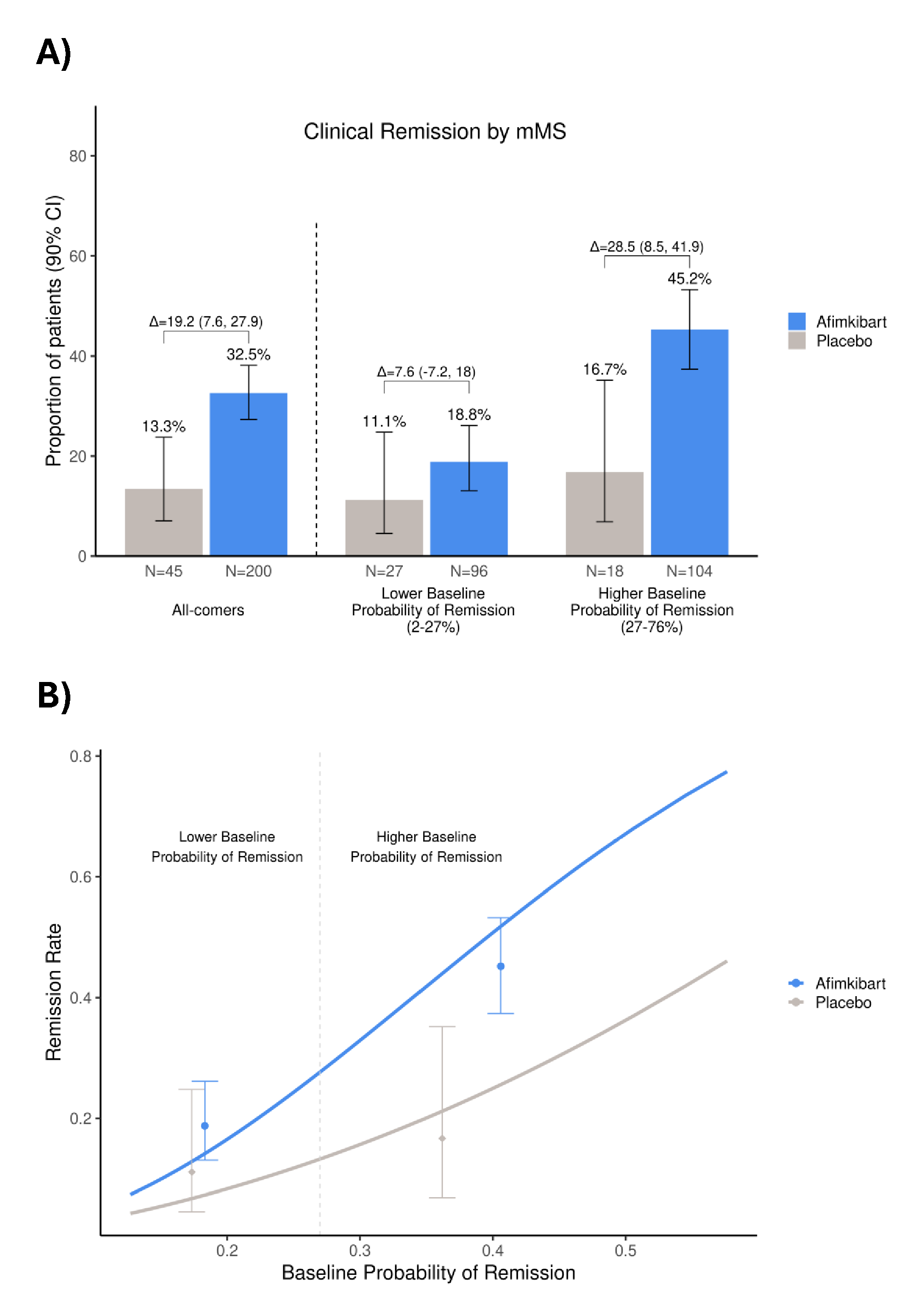
Jessica R.. Allegretti, MD, MPH1, Laurent Peyrin-Biroulet, MD, PhD2, Silvio Danese, MD, PhD3, Parambir S. Dulai, MD4, Anindita Banerjee, PhD5, Deepa E. Chandra, MPharm5, Elena Peeva, MD5, Srividya Neelakantan, PhD5, Michael S. Vincent, MD, PhD5, Kenneth Hung, MD, PhD5, Lyann Ursos, PhD6, Courtney Schiffman, PhD6, Daniela Bojic, MD, PhD7, Karen Lasch, MD6, Bruce E. Sands, MD, MS, FACG8 1Division of Gastroenterology, Hepatology, and Endoscopy, Brigham and Women’s Hospital, Harvard Medical School, Boston, MA; 2Department of Gastroenterology, CHRU Nancy, INSERM NGERE, Université de Lorraine, France, Vandœuvre-lès-Nancy, Lorraine, France; 3Gastroenterology and Endoscopy, IRCCS Ospedale San Raffaele and University Vita-Salute San Raffaele, Milan, Lombardia, Italy; 4Division of Gastroenterology and Hepatology, Feinberg School of Medicine, Northwestern University, Chicago, IL; 5Pfizer Inc., Cambridge, MA; 6Genentech, Inc., a member of the Roche Group, South San Francisco, CA; 7F. Hoffmann-La Roche Ltd, Basel, Basel-Stadt, Switzerland; 8Dr. Henry D. Janowitz Division of Gastroenterology, Icahn School of Medicine at Mount Sinai, New York, NY, USA, New York, NY Introduction: In the phase IIb TUSCANY-2 study (NCT04090411), afimkibart (RO7790121/RG6631), an anti-TL1A antibody, had a clinically meaningful effect in patients (pts) with moderate to severe ulcerative colitis. We report post hoc analyses of the relationship between baseline clinical characteristics and Week 14 (W14) efficacy in pts enrolled in TUSCANY-2. Methods: Pts were randomized to receive subcutaneous afimkibart 50mg, 150mg, 450mg or placebo (PBO) monthly during induction. In this analysis, afimkibart doses were pooled; the endpoint was clinical remission by modified Mayo score (mMS; defined as stool frequency subscore = 0/1; rectal bleeding subscore = 0; and endoscopic subscore = 0/1) at W14. Investigation of patient-specific treatment effects was guided by the risk modeling approach from the Predictive Approaches to Treatment effect Heterogeneity statement.1 We developed a regularized logistic regression model to predict the probability of W14 remission using baseline mMS, C-reactive protein (CRP), serum albumin, Robart’s Histopathology Index (RHI), number of failed advanced therapy classes, corticosteroid use, disease extent, disease duration, age and sex. The model was used to separate patients by baseline clinical characteristics to interrogate variation in treatment effects. Results: Overall, 32.5% of pts achieved clinical remission by mMS at W14 in the afimkibart arm (65/200; 90% CI 27.3–38.1) vs 13.3% (6/45; 90% CI 7.1–23.8) with PBO (treatment Δ 19.2%; 90% CI 7.6–27.9). Based on calibrated predictions from the multivariate model, all pts (PBO and afimkibart arms) had a 2–76% probability of W14 remission at baseline. On the clinically meaningful absolute scale, the treatment Δ in the top 50% of pts with a higher baseline probability of remission (27–76%) was 28.5% (90% CI 8–42; 45.2% afimkibart vs 16.7% PBO), versus a treatment Δ of 7.6% (90% CI –7–18; 18.8% afimkibart vs 11.1% PBO) in pts with a lower baseline probability of remission (2–27%; Figure). Lower baseline CRP, lower RHI and higher serum albumin contributed to a greater probability of remission and absolute benefit with afimkibart. Discussion: This analysis demonstrates how precision medicine approaches that simultaneously account for diverse baseline characteristics may improve interpretation of positive inflammatory bowel disease (IBD) clinical trial results. Integrating genetic and novel biomarkers with clinical features could help to better predict outcomes for pts with IBD.
1.Kent D, et al. Ann Intern Med 2020;172:35–45
Figure: Figure 1. The proportion of patients who achieved clinical remission by mMS, categorized by baseline probability of remission (A) the impact of baseline probability of clinical remission by mMS versus observed remission rate in patients (B)
Error bars represent A) 90% CI of the proportion of patients who achieved clinical remission B) 90% CI of the remission rate CI, confidence interval; mMS, modified Mayo Score

 photo")