P1066 - Efficacy and Safety of Guselkumab Through Week 96 After Intravenous or Subcutaneous Induction in Participants With Crohn’s Disease: Phase 3 Long-term Extension Data From GALAXI 2, GALAXI 3, and GRAVITI
University of Chicago Medicine Inflammatory Bowel Disease Center, Chicago, IL, USA Chicago, IL
Award: ACG Presidential Poster Award
Geert R. D’Haens, MD, PhD1, David T. Rubin, MD2, Anita Afzali, MD, MPH, MHCM3, Ailsa Hart, BA, BMBCh, PhD4, Tadakazu Hisamatsu, MD, PhD5, Nat A. Terry, MD, PhD6, Mobolaji Olurinde, MD, PhD6, Rian Van Rampelbergh, MD7, Jacqueline Yee, MS8, Wilbert van Duijnhoven, MSc7, Chris Corbett, MSc9, Elizabeth Merrall, MSc, PhD10, Qian Cao, MD, PhD11, Remo Panaccione, MD12, Julián Panés, MD13, Flavio Steinwurz, MD, MACG14, Silvio Danese, MD, PhD15, Bruce E. Sands, MD, MS, FACG16 1Department of Gastroenterology, Amsterdam University Medical Center, Amsterdam, Noord-Holland, Netherlands; 2University of Chicago Medicine Inflammatory Bowel Disease Center, Chicago, IL, USA, Chicago, IL; 3Department of Internal Medicine, Division of Digestive Diseases, University of Cincinnati College of Medicine, Cincinnati, OH, USA, Cincinnati, OH; 4London North-West University Healthcare NHS Trust, London, England, United Kingdom; 5Department of Gastroenterology and Hepatology, Kyorin University School of Medicine, Tokyo, Tokyo, Japan; 6Johnson & Johnson, Spring House, PA; 7Johnson & Johnson, Antwerp, Antwerpen, Belgium; 8Johnson & Johnson, Raritan, NJ; 9Johnson & Johnson UK, High Wycombe, England, United Kingdom; 10Johnson & Johnson, Leiden, Zuid-Holland, Netherlands; 11Sir Run Run Shaw Hospital Affiliated with School of Medicine, Zhejiang University, Hangzhou, Zhejiang, China; 12Inflammatory Bowel Disease Unit, Division of Gastroenterology and Hepatology, Department of Medicine, University of Calgary, Calgary, AB, Canada, Calgary, AB, Canada; 13Hospital Clínic de Barcelona, IDIBAPS, CIBERehd, Barcelona, Catalonia, Spain; 14Hospital Israelita Albert Einstein, São Paulo, Sao Paulo, Brazil; 15Gastroenterology and Endoscopy, IRCCS Ospedale San Raffaele and University Vita-Salute San Raffaele, Milan, Lombardia, Italy; 16Dr. Henry D. Janowitz Division of Gastroenterology, Icahn School of Medicine at Mount Sinai, New York, NY, USA, New York, NY Introduction: Guselkumab (GUS), a dual-acting IL-23p19 subunit inhibitor, is highly efficacious in participants (pts) with Crohn’s disease (CD). Phase 3 studies (GALAXI 2, GALAXI 3, and GRAVITI) showed that GUS administered via intravenous (IV) or subcutaneous (SC) induction followed by SC maintenance has similar efficacy after induction and through week (W)48. We report GUS W96 efficacy data from the long-term extension (LTE) periods of these studies and safety data from W0 to W96. Methods: The studies had double-blind, placebo-controlled, treat-through designs with blinding until the W48 database lock. GALAXI 2 and 3 evaluated IV GUS induction (200 mg at W0, W4, and W8) followed by SC maintenance (100 mg q8w or 200 mg q4w). GRAVITI assessed SC GUS induction (400 mg at W0, W4, and W8) and the same GUS maintenance regimens used in GALAXI. Pts entered the LTE receiving the treatment they received at W48. Between W52 and W80 (GALAXI only), pts on GUS 100 mg SC q8w who were not in clinical response received dose escalation to 200 mg SC q4w; pts on GUS 200mg SC q4w received a “sham" adjustment to GUS 200 mg SC q4w.
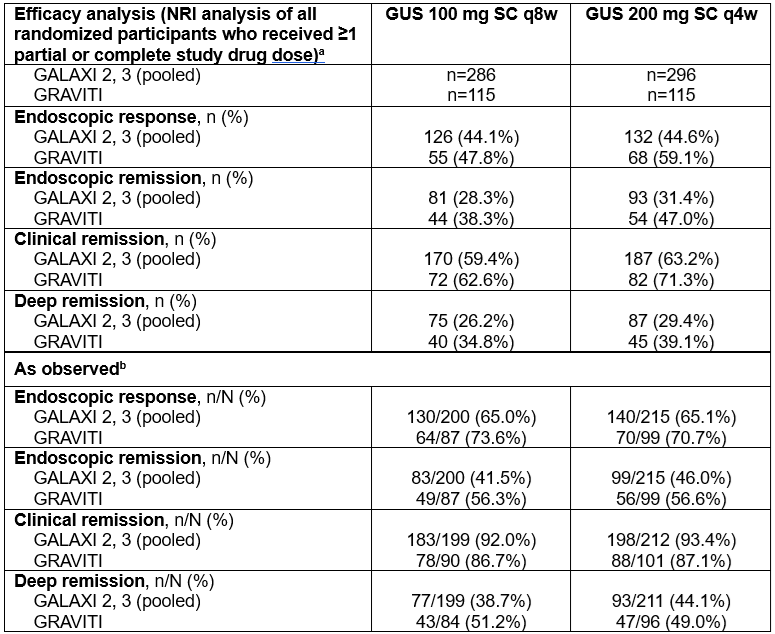
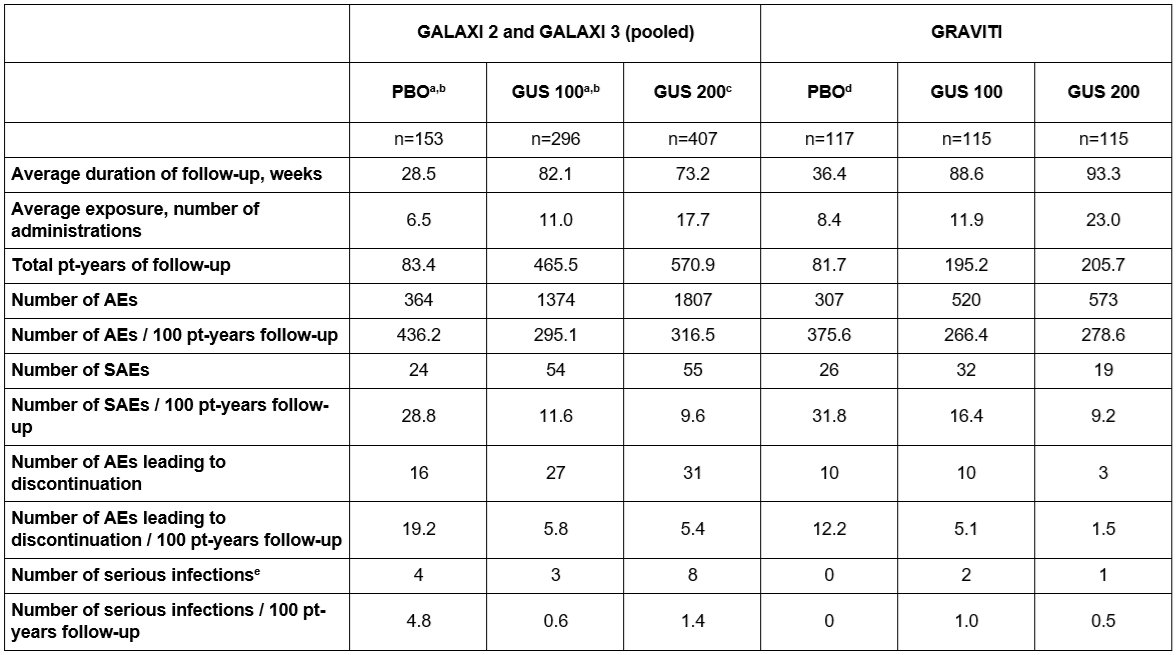
Efficacy analyses included all pts randomized at W0 with a Simple Endoscopic Activity Score for CD (SES-CD) ≥6 (≥4 for pts with isolated ileal disease) who received ≥1 study drug dose. Pts with missing data or who met treatment failure criteria were considered non-responders. As observed data are also presented. Safety analyses comprised all randomized pts who received study drug. Results: Between W0 and W96, 127/582 pts (21.8%) from GALAXI 2 and 3 and 31/230 pts (13.5%) from GRAVITI discontinued treatment. Across studies, high rates of long-term endoscopic response, endoscopic remission, clinical remission, and deep remission were observed after treatment with both GUS doses. Respective W96 rates for IV vs SC induction were 44.1% vs 47.8% (100 mg SC q8w) and 44.6% vs 59.1% (200 mg SC q4w) for endoscopic response, 28.3% vs 38.3% (100 mg SC q8w) and 31.4% vs 47.0% (200 mg SC q4w) for endoscopic remission, 59.4% vs 62.6% (100 mg SC q8w) and 63.2% vs 71.3% (200 mg SC q4w) for clinical remission, and 26.2% vs 34.8% (100 mg SC q8w) and 29.4% vs 39.1% (200 mg SC q4w) for deep remission (Table 1). Safety data through 2 years were comparable across studies and consistent with the safety profile of the label indications (Table 2). Discussion: Long-term efficacy outcomes show the durability of GUS treatment in CD through 2 years across multiple studies. No new safety concerns were identified.
Figure: Table 1. Number of Participants Reaching Clinical Endpoints at Week 96 in the Phase 3 GALAXI and GRAVITI Trials. a The efficacy analysis set for GALAXI included all randomized participants with a screening SES-CD ≥6 (≥4 for those with isolated ileal disease) who received ≥1 partial or complete study drug dose. The efficacy analysis set for GRAVITI included all randomized participants who received ≥1 dose of study intervention; an SES-CD ≥6 (≥4 for those with isolated ileal disease) was an entry criterion for GRAVITI. For the main efficacy analysis, non-responder imputation was used, for which missing data, discontinuations (including not entering the LTE), and CD-related intercurrent events (including dose adjustment in GALAXI) after the event were considered non-response. Meeting rescue criteria (at week 16 in GRAVITI) was not considered treatment failure. b The as observed analysis set included participants who entered the LTE, received ≥1 partial or complete study drug dose during the LTE, remained on treatment, and had data available at W96; participants who had a dose adjustment (GALAXI only) were not included at W96. Intercurrent events were not applicable. Endoscopic response was defined as a ≥50% improvement in SES-CD (GALAXI/GRAVITI) or an SES-CD ≤2 (GALAXI only). Endoscopic remission was defined as an SES-CD ≤4, with a ≥2-point reduction and no subscore >1 on any subcomponent. Clinical remission was defined as a CDAI score <150. Deep remission was defined as achieving both clinical remission and endoscopic remission, as defined above. CD=Crohn’s disease; CDAI=Crohn's Disease Activity Index; GUS=guselkumab; LTE=long-term extension; NRI=non-responder imputation; q4w=every 4 weeks; q8w=every 8 weeks; SC=subcutaneous; SES-CD=Simplified Endoscopic Activity Score for Crohn’s Disease.
Figure: Table 2. Summary of Treatment-Emergent Adverse Events Through Week 96 For All Randomized Participants Who Received ≥1 Study Drug Dose a Up to dose adjustment. b Treatment group at the start of the long-term extension period. Includes events for participants who dose adjusted from week 48 up to the time point of dose adjustment, and all events from week 48 through week 96 for participants who never dose adjusted. c Participants who were randomized to receive GUS 200 mg SC q4w maintenance dosing, or had a dose adjustment (including "sham") to GUS 200 mg SC q4w dosing from all treatment groups (including those randomized to placebo and ustekinumab); for participants who had a dose adjustment, only data after their first GUS 200 mg dose are included. d Includes all placebo participants, excluding data after GUS rescue. e Infections are based on MedDRA system organ class “Infections and Infestations.” Adverse events are coded using MedDRA Version 27.0. AE=adverse event; GUS=guselkumab; MedDRA=Medical Dictionary for Regulatory Activities; PBO=placebo; pt=patient; SAE=serious adverse event.