Abdul Adnan Vhora, BS1, Benjamin Schwartz, MD2, Neil Kapil, MD2 1Rush University Medical Center, Harvey, IL; 2Rush University Medical Center, Chicago, IL Introduction: Refractory gastrointestinal (GI) bleeding is characterized by recurrent or persistent blood loss despite initial evaluation and therapy. Most bleeding is identified with upper and lower endoscopy. However, less than 5% of the time, bleeding occurs from the small bowel and requires additional evaluation and intervention. In patients with Crohn’s disease, identifying the bleeding source becomes more complex due complex anatomy, prior surgeries, and intermittent inflammation. Mucosal ulcerations are a common source of Crohn’s related bleeding, although the differential should remain broad.
Case Description/
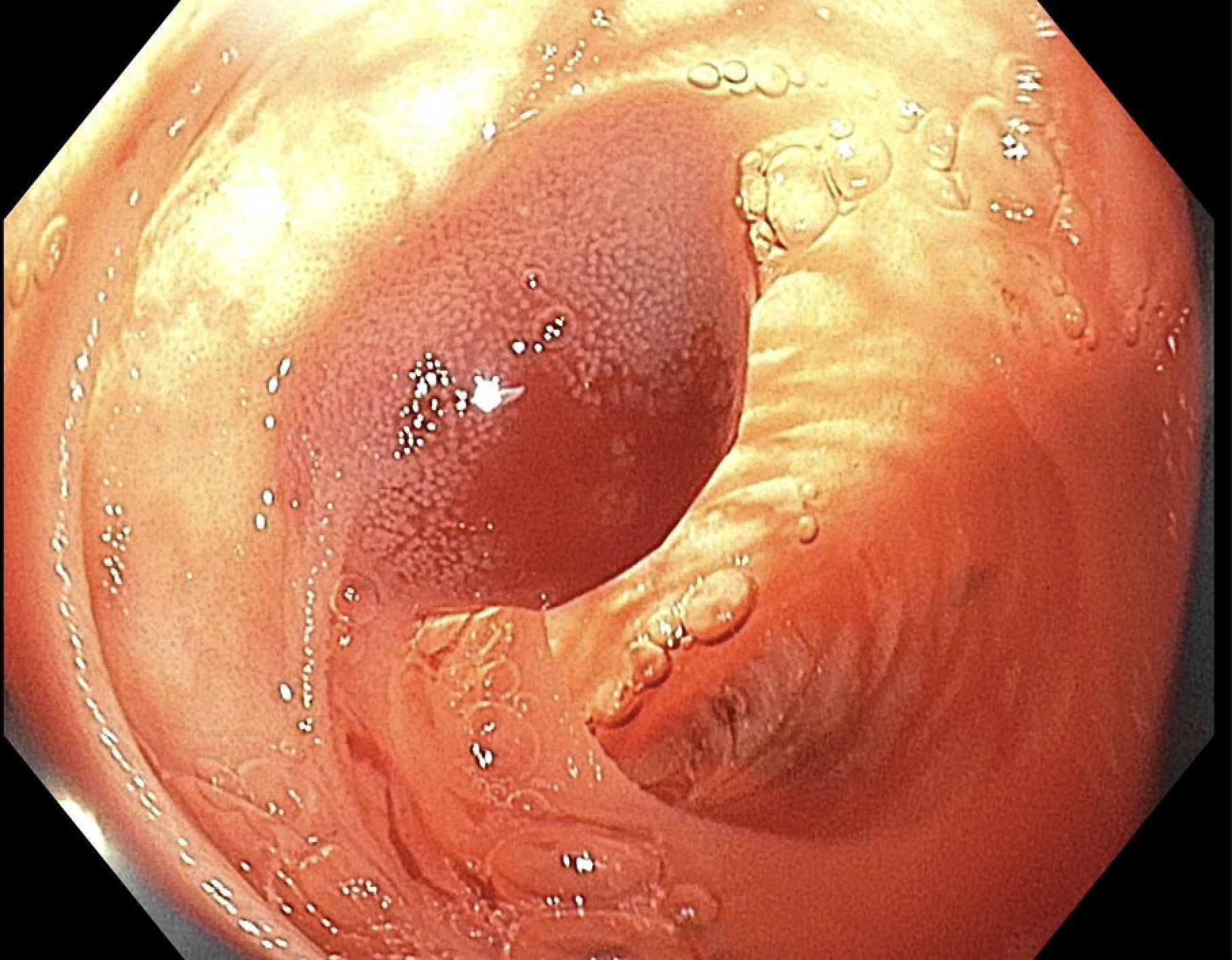
Methods: A 48-year-old woman with Crohn's disease now in remission with prior small bowel resections and ileocecectomy presented to the hospital with black stools with subsequent bright red blood. She was acutely anemic. Prior admission for rectal bleeding and anemia identified a jejunal lesion on video capsule endoscopy (VCE). Repeat VCE was performed which showed active mid small bowel bleeding. Antegrade double balloon enteroscopy (DBE) did not identify bleeding. Retrograde DBE treated small non-bleeding angioectasias without identifying a culprit lesion. Due to ongoing bleeding and persistent transfusion requirements, intraoperative enteroscopy was pursued which identified a hemorrhagic lesion 50 cm distal to a tattoo at the maximum extent of prior enteroscopy but was not amenable to endoscopic treatment. Due to extensive adhesions, the surgery was converted to open laparotomy. An actively bleeding jejunal lesion was identified and resected. Pathology revealed benign vascular proliferation without active inflammation. The patient reported resolution of rectal bleeding and symptomatic improvement. Her hemoglobin stabilized above 12g/dL. Discussion: Benign vascular jejunal lesions are a rare cause of obscure GI bleeding. While these lesions are often clinically silent, they can lead to iron-deficiency anemia or intermittent bleeding. VCE is essential in localizing culprit lesions which can then be treated via DBE. However, in patients with extensive surgeries and history of complicated inflammatory disease, these minimally invasive options have limitations. When VCE identifies a small bowel lesion that cannot be reached with DBE, intraoperative enteroscopy can be invaluable in evaluation and definitive treatment. This multimodal and multidisciplinary approach was essential in identifying and treating this rare cause of refractory GI bleeding in a patient with Crohn’s.
Disclosures: Abdul Adnan Vhora indicated no relevant financial relationships. Benjamin Schwartz indicated no relevant financial relationships. Neil Kapil indicated no relevant financial relationships.
Abdul Adnan Vhora, BS1, Benjamin Schwartz, MD2, Neil Kapil, MD2. P1007 - Refractory GI Bleeding From a Benign Jejunal Vascular Proliferation Requiring Intraoperative Enteroscopy and Surgical Resection, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.