SUNY Upstate Medical University Hospital Syracuse, NY
Randa Elzein, MBBS, Idan Goren, MD, Azhar Hussain, MBBS SUNY Upstate Medical University Hospital, Syracuse, NY Introduction: Gastrostomy tubes are regularly used for long-term enteral feeding, yet serious mechanical complications remain infrequent. We report a unique case of a percutaneous endoscopic gastrostomy (PEG) tube causing functional gastric outlet obstruction (GOO) and a Forrest IIa ulcer with a non-bleeding visible vessel.
Case Description/
Methods: A 71-year-old male with alcoholic cirrhosis, head and neck cancer (s/p PEG), and multiple comorbidities presented with melena and blood refluxing into his G-tube after seemingly reinserting the partially dislodged tube himself. He was found to be hypotensive and profoundly anemic (hemoglobin 6.6 g/dL). CTA abdomen/pelvis shown the PEG tube tip and balloon projecting into the duodenum, but no active bleeding was seen. Esophagogastroduodenoscopy (EGD) confirmed the PEG balloon had migrated across the pylorus, causing mechanical GOO and a 7 mm gastric ulcer at the incisura with a non-bleeding visible vessel (Forrest IIa). The balloon had eroded the gastric wall, embedding into the mucosa and causing pressure ulceration. Two hemostatic clips were placed effectively, and the PEG tube was deflated and repositioned within the gastric lumen (3.5 cm at skin level), resolving the obstruction. The esophagus revealed a benign, traversable stenosis, and no varices were present. Discussion: PEG-induced GOO with concomitant ulceration and potential bleeding is an unusual but significant complication that may not be apparent on imaging. Early endoscopic evaluation is essential in patients with gastrointestinal bleeding and PEG dysfunction, particularly when history suggests malposition. Clinicians should maintain a high index of suspicion for mechanical causes of bleeding, specifically when Forrest IIa lesions are present. This case highlights the value of timely endoscopic therapy, proper PEG maintenance, and detection of atypical bleeding sources in high-risk patients.
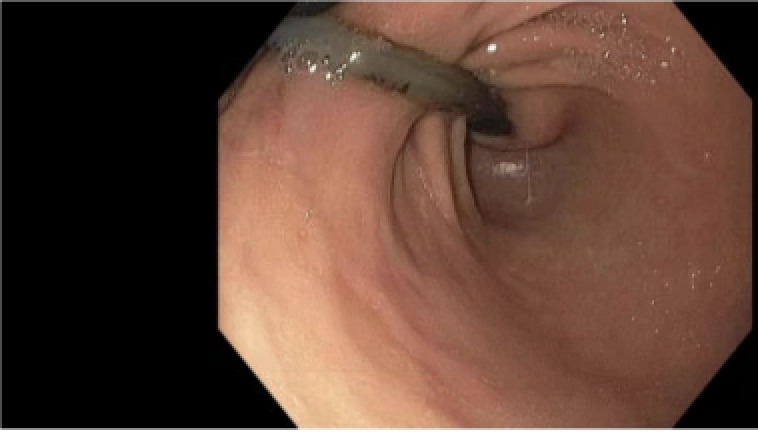
Figure: Endoscopic image showing migrated PEG tube balloon across the pylorus causing mechanical gastric outlet obstruction.
Figure: Gastric ulcer at the incisura with non-bleeding visible vessel (Forrest IIa) caused by pressure necrosis from migrated PEG balloon.
Disclosures: Randa Elzein indicated no relevant financial relationships. Idan Goren indicated no relevant financial relationships. Azhar Hussain indicated no relevant financial relationships.
Randa Elzein, MBBS, Idan Goren, MD, Azhar Hussain, MBBS. P1004 - PEG-Induced Gastric Outlet Obstruction and Forrest IIa Ulcer: A Rare but Reversible Cause of GI Bleeding, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.