Douglas Rivera Agosto, DM1, Suhail Kayyali, DO2, Shivani Trivedi, DO2, Marc Kudelko, DO2 1HCA Florida Largo Hospital, Bradenton, FL; 2HCA Florida Largo Hospital, Largo, FL Introduction: In this report we describe the unique case of an upper GI bleed caused by a Dieulafoy lesion located within a windsock diverticulum. This case highlights the importance of considering congenital duodenal anomalies in patients with obscure or recurrent upper GI bleeding & emphasizes the diagnostic value of meticulous endoscopic evaluation in atypical presentations.
Case Description/
Methods: 70-year-old female presented to the ED with complaints of palpitations and chest discomfort. Her medical history was significant for iron deficiency anemia, gastroesophageal reflux disease (GERD). Initial laboratory revealed hemoglobin level of 6.9 g/dL. The patient also reported passing dark-colored stools. She received blood transfusions and was medically stabilized, including undergoing a cardiac evaluation. She subsequently underwent EGD with enteroscopy. Endoscopic examination revealed altered upper gastrointestinal anatomy, characterized by a double lumen appearance. Closer inspection identified findings consistent with a Windsock duodenal diverticulum. Within this area, fresh blood was visualized. Careful evaluation uncovered a 1 mm Dieulafoy lesion with active bleeding. Endoscopic intervention was performed, and hemostasis was successfully achieved. Discussion: Therapeutically, management of Dieulafoy lesions typically involves endoscopic techniques such as injection therapy, hemoclips, and thermal coagulation. However, lesions within a windsock diverticulum may pose technical limitations due to restricted access, risk of perforation, and impaired visualization. In our case, hemostasis was successfully achieved using epinephrine injection, gold probe and clipping, with no recurrent bleeding on follow-up. However, in cases where endoscopic control is not feasible, angiographic embolization or surgical resection may be necessary.
Given the extreme rarity of this presentation, we propose that clinicians remain vigilant for such anatomical anomalies, particularly when standard endoscopic evaluations fail to reveal a clear source of bleeding. Furthermore, this case expands the known spectrum of Dieulafoy lesion locations and highlights the potential for complex interplay between congenital GI tract anomalies and vascular malformations.
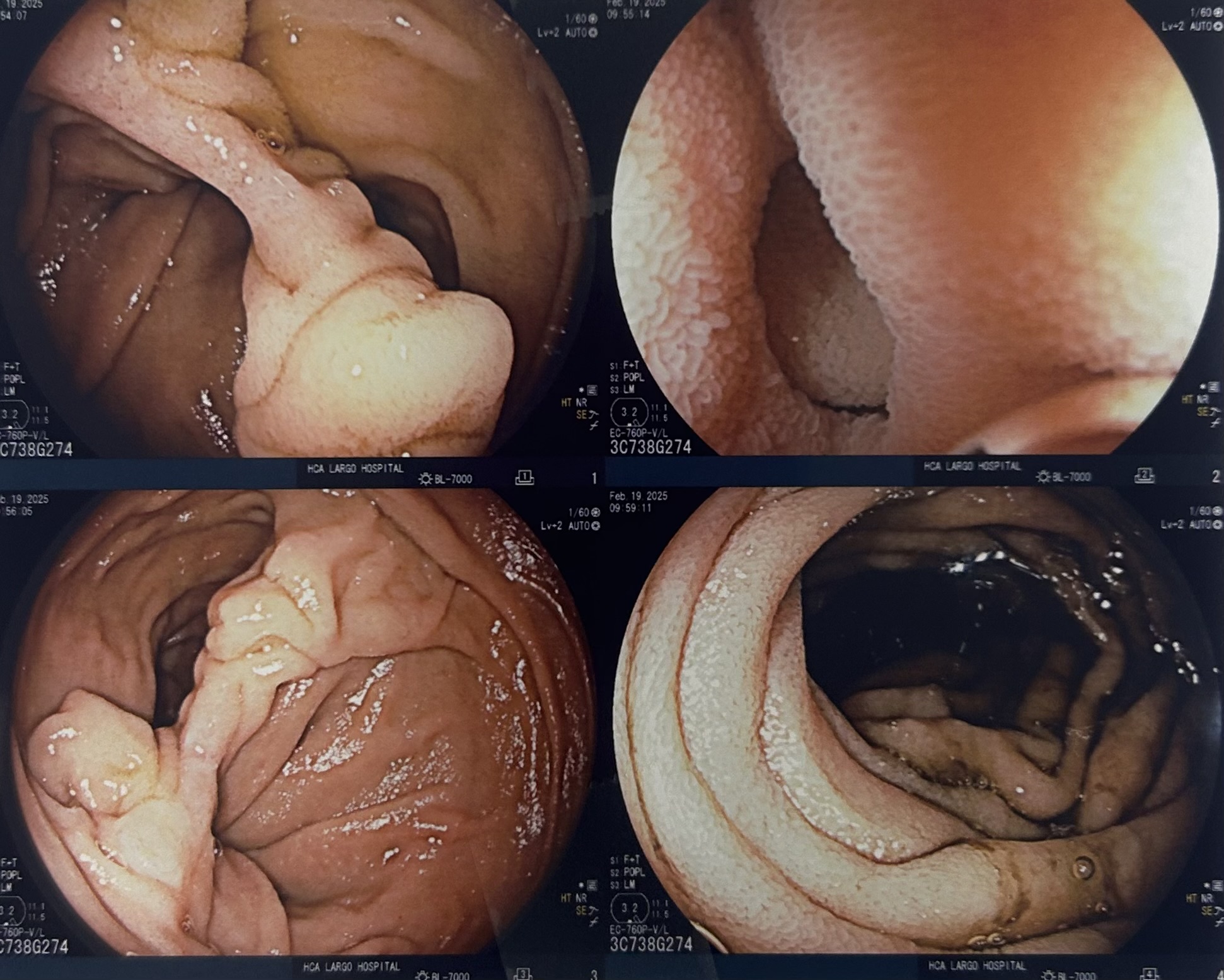
Figure: Altered upper gastrointestinal anatomy characterized by a double lumen appearance in the duodenum
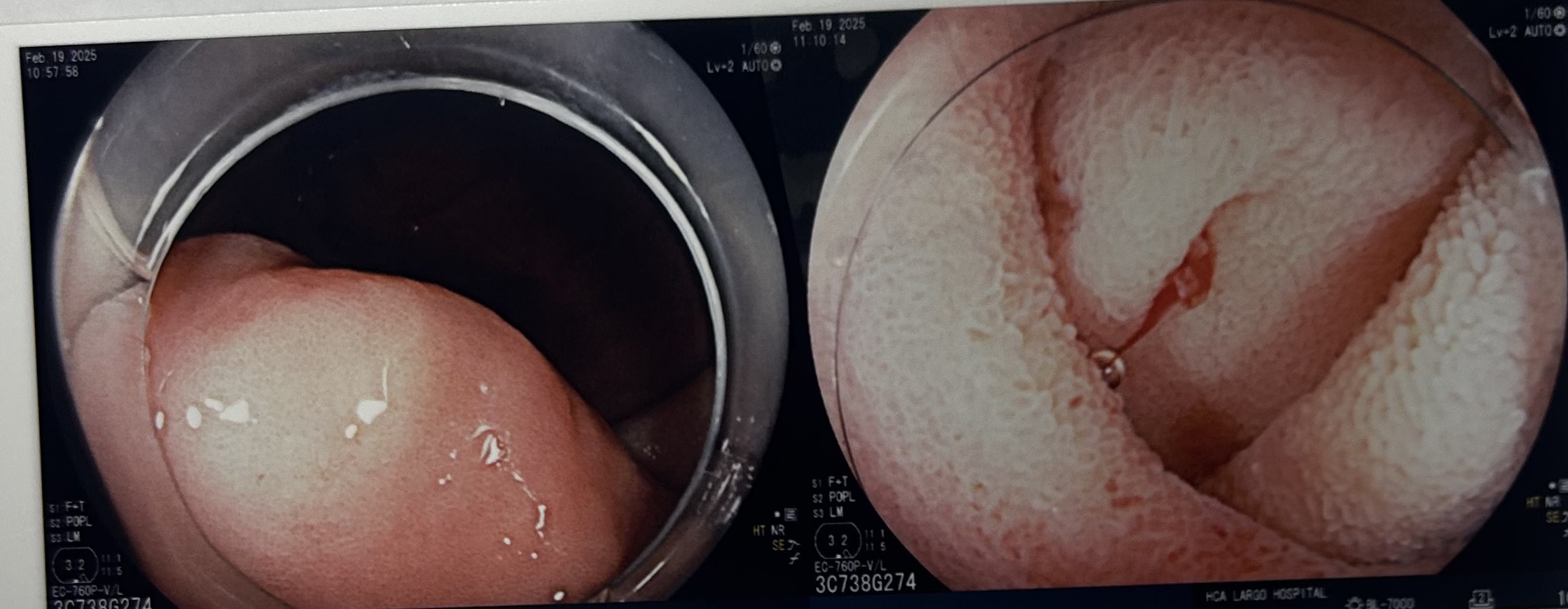
Figure: Dieulafoy lesion noted on Right sided image
Disclosures: Douglas Rivera Agosto indicated no relevant financial relationships. Suhail Kayyali indicated no relevant financial relationships. Shivani Trivedi indicated no relevant financial relationships. Marc Kudelko indicated no relevant financial relationships.
Douglas Rivera Agosto, DM1, Suhail Kayyali, DO2, Shivani Trivedi, DO2, Marc Kudelko, DO2. P0996 - Upper GI Bleed from a Dieulafoy Lesion Within a Duodenal Windsock Diverticulum, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

.jpg "Douglas Rivera Agosto, DM photo")