Piedmont Athens Regional Medical Centre Athens, GA
Samuel Acheampong, MD1, Patrick Berchie, MD1, Prince Darko, MD1, Eunice Omeludike, MD1, Elizabeth Soladoye, MD, MPH2, George Annan, MD1, Dominic Ofosu-Amakye, MD1 1Piedmont Athens Regional Medical Centre, Athens, GA; 2Piedmont Athens Regional, Athens, GA Introduction: Gastrointestinal (GI) bleeding is a rare but serious complication following Roux-en-Y gastric bypass (RYGB) surgery. While early postoperative bleeding is more commonly reported, late-onset bleeding is a much rarer and potentially life-threatening event. Marginal ulcers, occurring at the gastrojejunal anastomosis, are a recognized cause of late GI bleeding. We discuss a 38-year-old male presenting with significant GI bleeding four years post-RYGB.
Case Description/
Methods: A 38-year-old male who presented with upper GI bleeding four years post-RYGB. He had a history of chronic alcohol use. The patient experienced melena for a week. Upon admission, he was stable, and laboratory findings revealed a hemoglobin level of 9.8 g/dL, white blood cell count of 5.2, platelet count of 294, and an international normalized ratio (INR) of 1.16. His Glasgow-Blatchford score was 10, signaling a high risk for GI bleeding.
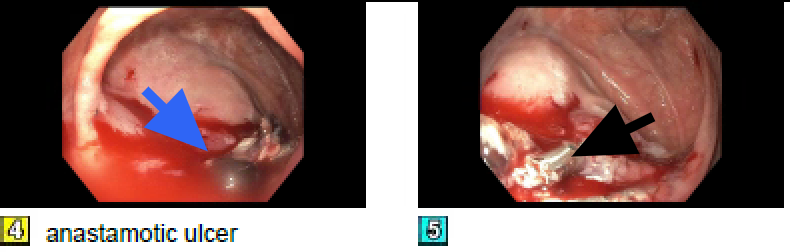
Computed Tomography (CT) imaging showed diffuse fatty liver infiltration, mild non-specific panniculitis, and prior bariatric surgery changes. Endoscopic evaluation confirmed a gastrojejunal ulcer at the anastomosis site, displaying congestion, edema, erythema, and ulceration. Endoscopy revealed a Roux-en-Y gastrojejunostomy ulcer with congestion and erythema at the gastrojejunal anastomosis (fig 4). Hemostasis was achieved via: epinephrine injection (4 mL, 0.2 mg/mL), placement of two hemostatic clips and hemostatic spray application (fig 5). A unit of packed red blood cells was transfused. The patient tested positive for H. pylori and was discharged on quadruple therapy with outpatient follow-up Discussion: GI bleeding post RYGB can be early(1-4%incidence) or late( >30 days). Typically arises from marginal ulcers at the gastrojejunal site which account for 0.6 to 16% of cases. Risk factors include smoking, NSAID use, diabetes, and H. pylori infection. Late bleeding sources include the Roux limb(hematochezia) or gastric remnant/duodenum(melena). Alcohol use disorder in our patient likely increased his chance.
Late GI bleeding following RYGB, although rare, is potentially life-threatening. Timely endoscopic intervention combined with long-term medical management is essential for recurrence prevention. Identifying marginal ulcers and understanding risk factors remain crucial for optimizing patient outcomes.
Figure: Image 4 with blue arrow showing bleeding gastric Ulcer.
Image 5 with black arrow showing bleeding Ulcer with hemostatic clip.
Disclosures: Samuel Acheampong indicated no relevant financial relationships. Patrick Berchie indicated no relevant financial relationships. Prince Darko indicated no relevant financial relationships. Eunice Omeludike indicated no relevant financial relationships. Elizabeth Soladoye indicated no relevant financial relationships. George Annan indicated no relevant financial relationships. Dominic Ofosu-Amakye indicated no relevant financial relationships.
Samuel Acheampong, MD1, Patrick Berchie, MD1, Prince Darko, MD1, Eunice Omeludike, MD1, Elizabeth Soladoye, MD, MPH2, George Annan, MD1, Dominic Ofosu-Amakye, MD1. P0957 - Upper GI Bleeding Post Roux-en-Y Gastric Bypass, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.