University of Iowa Hospitals & Clinics Iowa City, IA
Robert Schoeneich, MD1, Joseph Brant, MD2, Rintaro Hashimoto, MD1 1University of Iowa Hospitals & Clinics, Iowa City, IA; 2University of Iowa, North Liberty, IA Introduction: A Meckel’s diverticulum (MD) originates from incomplete closure of the vitelline duct during gestation. Classically, it follows the “rule of 2’s”: occurring in 2% of the population, >2:1 male-to-female ratio, 2% risk of complications, located 2 feet from the ileocecal valve (ICV), 2 inches long, 2 types of ectopic tissue (gastric or pancreatic), and usually presents by age 2. Most commonly a MD presents as painless hematochezia. Histologically, bleeding diverticula are found to have ectopic gastric mucosa in 75% of cases with associated acid-induced ulceration. We present a challenging diagnosis of MD in an adult.
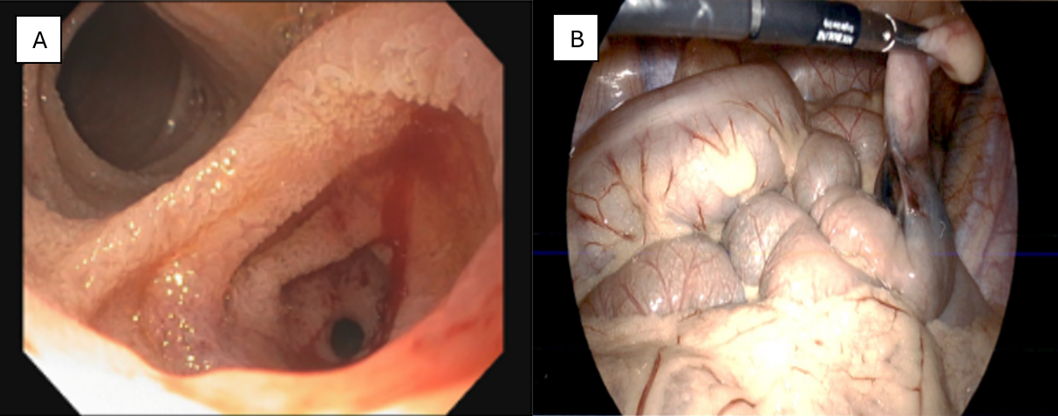
Case Description/
Methods: A 19-year-old male presented with hematochezia and syncope with associated hemoglobin decline of 13 to 9.3 g/dL. Colonoscopy showed blood throughout the colon and terminal ileum (TI) without identified culprit lesion. Upper endoscopy was without abnormality. Subsequent computed tomography angiography showed no active extravasation. Capsule endoscopy showed fresh blood arising within the ileum without clear culprit. A Meckel scan showed transient focus of activity in right lower quadrant, but was negative for ectopic gastric mucosa. Lower double balloon enteroscopy (DBE) revealed a double lumen with active bleeding from a stenosed diverticular inlet (Figure 1A) ~60 cm from the ICV. The patient underwent surgical resection of the diverticulum (Figure 1B) with operative pathology confirming a MD with ectopic gastric mucosa. Discussion: This case highlights the challenge in securing a preoperative diagnosis particularly in an adult with MD. Our patient had numerous nondiagnostic studies including a Meckel scan prior to receiving a diagnosis. A Meckel scan utilizes a radiotracer (technetium-99m pertechnetate) taken up by ectopic gastric mucosa and otherwise is nondiagnostic with ectopic pancreatic tissue. Sensitivity is lower (62.5%) in adults possibly due to insufficient ectopic gastric mucosa to accumulate radiotracer, which may also account for their later presentation. Additionally, the scan may be falsely negative during active hemorrhage due to radiotracer dilution or autoregulatory vasoconstriction by mesenteric vasculature. Administering H2 blockers, pentagastrin, proton pump inhibitors, or glucagon prior to the scan may increase yield. DBE is not routinely pursued but may serve a role when other studies are nondiagnostic. Ultimately, it is important to not be dissuaded by nondiagnostic studies and maintain a high index of clinical suspicion.
Figure: Figure 1: A) Image from lower DBE showing double lumen with bleeding from stenosed diverticulum. B) Intraoperative image showing diverticulum near tattooed small intestine.
Disclosures: Robert Schoeneich indicated no relevant financial relationships. Joseph Brant indicated no relevant financial relationships. Rintaro Hashimoto indicated no relevant financial relationships.
Robert Schoeneich, MD1, Joseph Brant, MD2, Rintaro Hashimoto, MD1. P0949 - The Challenge of a Preoperative Diagnosis in an Adult With Meckel’s Diverticulum, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")