University of Medicine and Health Sciences Clinton Township, MI
Jeffrey Sharza, BS1, Rama Aljundi, MD2, Yunus Teken, DO2, Hana Raza, MD2, Ali Daoud, MD2, Bashar Hammad, MD2, Kyle Antosiek, DO2, Mohanand Suede, MD2 1University of Medicine and Health Sciences, Clinton Township, MI; 2McLaren Oakland Hospital, Pontiac, MI Introduction: Choriocarcinoma is an aggressive variant of testicular cancer that may seed hematogenously. It primarily invades the lungs or brain. In this vignette we investigate an exceedingly rare metastatic pattern in the jejunum resulting in persistent blood loss refractory to blood transfusion.
Case Description/
Methods: A 23-year-old male with no past medical history presented to the emergency department after experiencing dizziness and near syncope for 3 days. The patient, who immigrated to the United States from Guatemala 2 years ago and lacks an established primary care provider, initially experienced these symptoms at his construction job. He endorsed occasional bouts of painless bloody stools. He denies drinking alcohol or smoking cigarettes. Vital signs on arrival revealed sinus tachycardia. Laboratory evaluation demonstrated significant anemia with a hemoglobin of 5.3 g/dL. An Rh O-negative blood transfusion was initiated, and further hematologic workup was ordered. CT imaging revealed a large right testicular mass and concerning lung metastases, and no active GI bleed. Physical exam confirmed an enlarged right testicle the patient believed was a hernia for 6 months. The patient was admitted to the ICU with critical care, oncology, and gastroenterology consultations. A urine beta-hCG was elevated at 12,296 mIU/mL and fetoprotein was 146 ng/mL indicative of metastatic mixed germ cell carcinoma. Despite multiple units of packed red blood cells, his hemoglobin remained low. Upper endoscopy biopsies were negative for active bleeding. Colonoscopy showed severe melena warranting a second upper endoscopy with push enteroscopy and identified an atypical jejunal mass that was actively hemorrhaging and biopsied. Histopathology confirmed germ cell metastasis likely secondary to choriocarcinoma. Immunohistochemistry confirmed the diagnosis. Discussion: Choriocarcinoma is a nonseminomatous germ cell tumor characterized by its aggressive nature to metastasize and potential to cause fatal hemorrhage. The most implicated sites of distant metastasis include the lungs, brain and liver, while the small bowel is very rare. Our patient highlights the unpredictable nature of choriocarcinoma metastasis and emphasizes the importance of maintaining a high index of suspicion for unusual metastatic sites in patients with choriocarcinoma, particularly when faced with persistent and unexplained gi bleeding. Thorough endoscopic evaluation, including push enteroscopy, may be necessary to address these challenging locations.
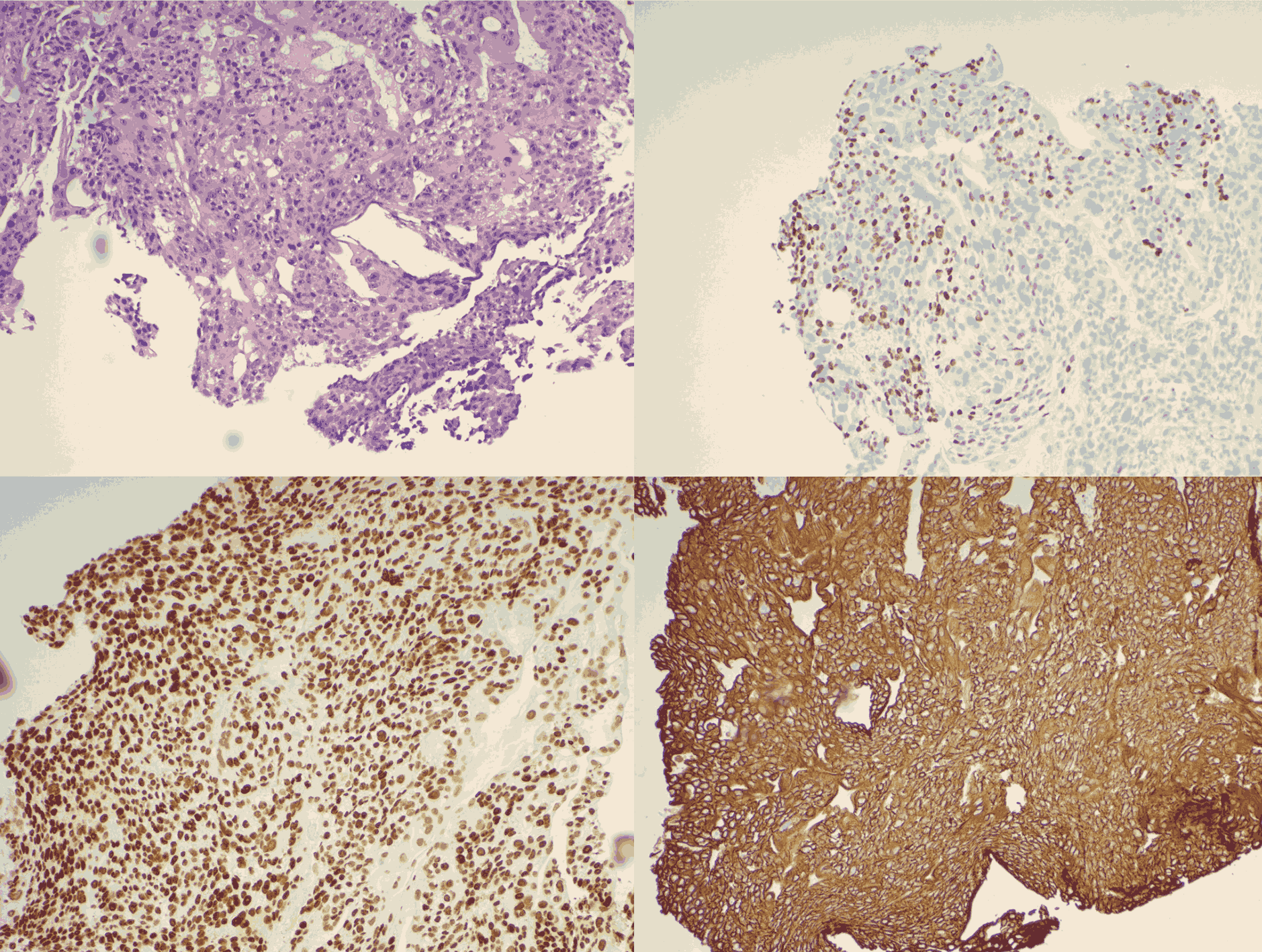
Figure: Biopsy of small bowel mass. HE (top left) and positive staining for Sall4 (top right), Gata3 (bottom left) and CK AE1/3 (bottom right). Positive staining of these markers, but negative for others confirm the choriocarcinoma component.
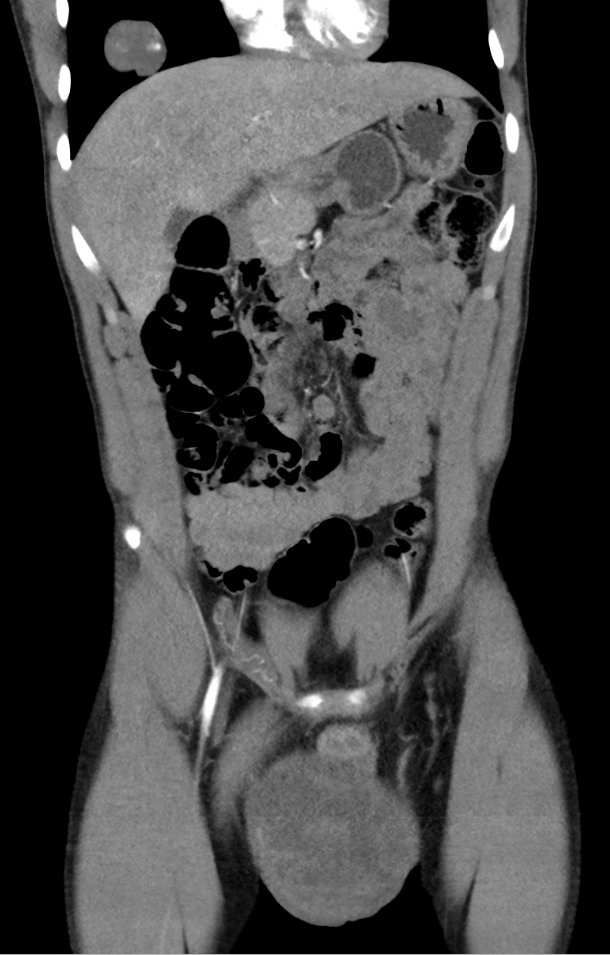
Figure: CT Abdomen/Pelvis: Lung nodules, large right testicular mass (at least 12 x 10 cm), and horseshoe kidney without hydronephrosis.
Disclosures: Jeffrey Sharza indicated no relevant financial relationships. Rama Aljundi indicated no relevant financial relationships. Yunus Teken indicated no relevant financial relationships. Hana Raza indicated no relevant financial relationships. Ali Daoud indicated no relevant financial relationships. Bashar Hammad indicated no relevant financial relationships. Kyle Antosiek indicated no relevant financial relationships. Mohanand Suede indicated no relevant financial relationships.
Jeffrey Sharza, BS1, Rama Aljundi, MD2, Yunus Teken, DO2, Hana Raza, MD2, Ali Daoud, MD2, Bashar Hammad, MD2, Kyle Antosiek, DO2, Mohanand Suede, MD2. P0947 - A Case Report of Anemia Secondary to Atypical Testicular Carcinoma Metastasis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.