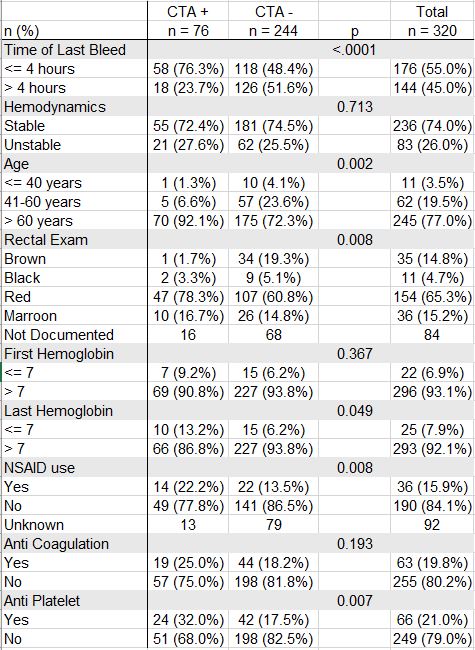
Julianna Tantum, DO, Lauren Davis, DO, Erin Hollis, DO, Mark McGarrey, MD, Henry Burke, DO, Stephanie Kjelstrom, PhD, Nicole Albert, DO Lankenau Medical Center, Wynnewood, PA Introduction: Colonoscopy is the diagnostic test of choice for lower GI bleeding (LGIB) but has limited therapeutic abilities. Computed tomography angiogram (CTA) is suggested as the initial diagnostic test in patients with hemodynamically significant hematochezia. However, CTA has a low yield when bleeding has stopped. The purpose of this study was to evaluate the positivity rate of CTA in cases of LGIB in the ED at Lankenau Medical Center (LMC). Methods: This was a retrospective chart review on patients that had a CTA for LGIB from January 2021–January 2024 while in the ED at LMC. Patients were excluded if they underwent CTA for reasons other than GIB, upper or small bowel bleeding, or if time of last bleed was unknown. CTA results, time of last bleed, rectal exam, hemodynamics, hemoglobin values, NSAID use, anti-coagulation, and anti-platelet therapy were extracted. Patients were grouped as positive or negative CTA. A positive CTA was defined as active bleeding within the colon. Patients were further grouped based on time from bleed to CTA (≤ 4 hours or >4 hours), hemodynamic stability (stable: SBP≥ 90 mmHg and HR < 100 BPM), age (age < 40, 41- 60, >60), rectal exam (brown, black, red, maroon), first hemoglobin on arrival to the ED and hemoglobin prior to CTA (Hgb ≤7 or > 7), NSAID use, anti-coagulation/anti-platelet therapy use. Statistical analysis was performed. Results: A total of 320 patients were included in the study with 76 positive and 244 negative CTAs. CTAs were more likely to be positive when patient bled ≤ 4 hours from time CTA was done (76.3 % vs 48.4%, p < 0.0001). Notable differences were also found between age, last hemoglobin before CTA, NSAID use, and use of anti-platelets. There was no difference for hemodynamics, first hemoglobin, and anti-coagulation use (Table 1). The best predictors of a positive CTA were ≤ 4 hours from last bleed (OR 3.2 (1.7, 5.8)), > 60 years of age (OR 3.4 (1.4, 8.5)), and the use of anti-platelets based on a multivariable logistic regression analysis. Discussion: The positivity rate of CTAs for LGIB was highest in patients who bled within 4 hours of the CTA. Additional factors including age > 60 and use of anti-platelet agents were also predictors of a positive CTA. This study concludes that careful selection of patients for CTA in cases of LGIB is required and supports established guidelines that CTAs should be obtained to localize bleeding in patients with hemodynamically significant bleeding within a 4-hour timeframe.
Figure: Table 1. Demographics and patient characteristics compared by CTA status.
Disclosures: Julianna Tantum indicated no relevant financial relationships. Lauren Davis indicated no relevant financial relationships. Erin Hollis indicated no relevant financial relationships. Mark McGarrey indicated no relevant financial relationships. Henry Burke indicated no relevant financial relationships. Stephanie Kjelstrom indicated no relevant financial relationships. Nicole Albert indicated no relevant financial relationships.
Julianna Tantum, DO, Lauren Davis, DO, Erin Hollis, DO, Mark McGarrey, MD, Henry Burke, DO, Stephanie Kjelstrom, PhD, Nicole Albert, DO. P0921 - Examining CT Angiography Positivity Rates in Lower GI Bleeding in the Emergency Department at Lankenau Medical Center, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.