Warsha Korani, MD1, Arham Siddiqui, 2, Fatmaelzahraa Abdelfattah, MD3, Adel Farhoud, MD4 1Conemaugh Memorial Medical Center, Johnstown, PA; 2University of Texas Health San Antonio, San Antonio, TX; 3Mayo Clinic, Phoenix, AZ; 4Concord Hospital, Concord, NH Introduction: Retroperitoneal fibrosis (RF) is a rare condition often associated with IgG4-related disease (RD), presenting with nonspecific symptoms and diagnosed primarily through imaging. While traditionally considered idiopathic, growing evidence suggests many cases are manifestations of IgG4-RD, underscoring the importance of serologic and histopathologic evaluation.We present a rare case of gastric outlet obstruction (GOO) secondary to IgG4-related RF
Case Description/
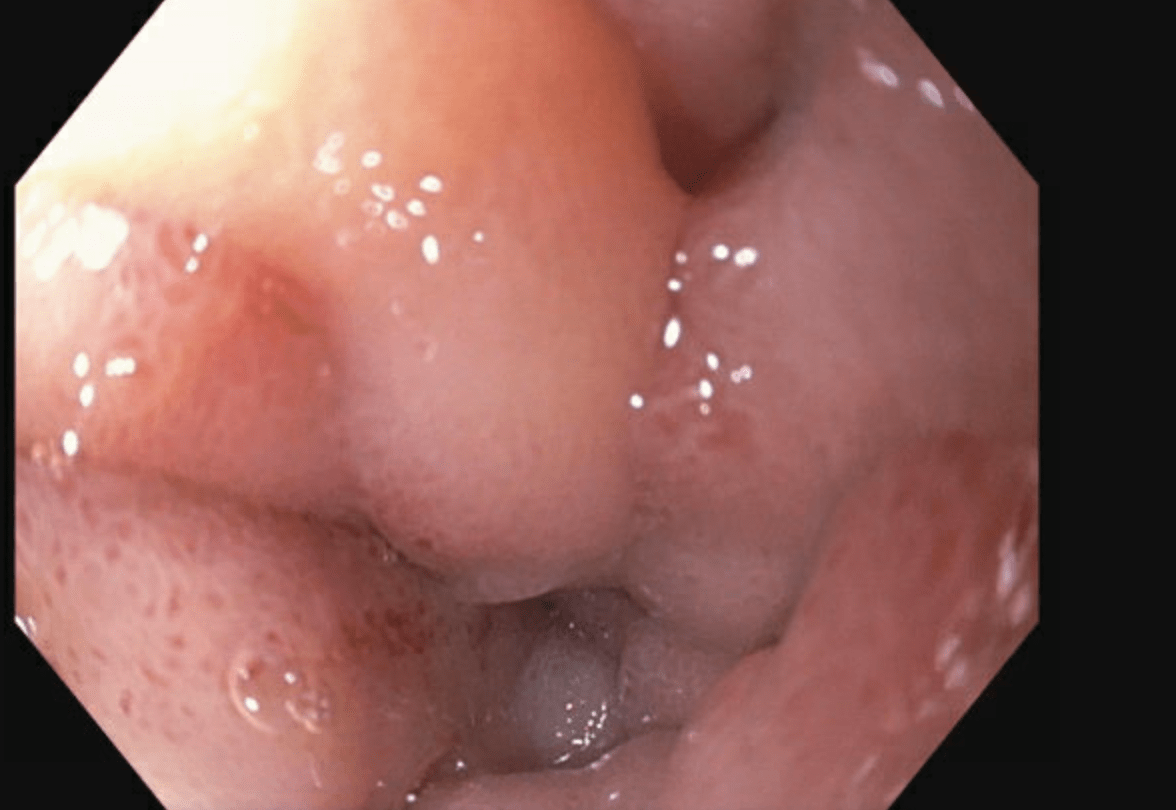
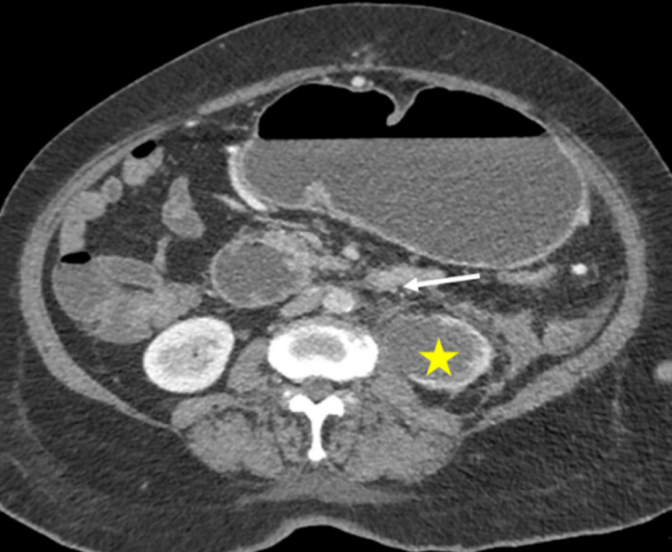
Methods: A 73-year-old male with a history of recently diagnosed IgG4-RD presented with 3 days of nausea, vomiting, abdominal pain, and a 20-pound unintentional weight loss over several months. CT imaging revealed a markedly dilated, fluid-filled stomach concerning for GOO, along with inflammatory changes in the terminal ileum and cecum. NG tube was placed for decompression; however, the placement was traumatic and resulted in blood-tinged output.Gastroenterology was consulted, and the patient underwent EGD for further evaluation. This showed a mucosal defect in the lower esophagus with associated clot, managed with endoscopic clipping and epinephrine injection. There was significant edema and erythema in the duodenal sweep, with difficulty advancing the scope. The second and third portions of the duodenum appeared normal. Biopsies from the duodenal sweep revealed mild duodenopathy and this was felt to be more reactive inflammation.As biopsies were non-diagnostic, prior CT imaging was re-reviewed, which demonstrated subtle infiltrative retroperitoneal soft tissue thickening consistent with RF with a normal appearing pancreas. This fibrosis extended along the ureters and had previously caused bilateral hydronephrosis requiring nephrostomy tubes. Based on these imaging findings and lack of other etiologies, the patient’s GOO was attributed to duodenal compression from IgG4-related RF. Discussion: IgG4-RD can mimic malignancy or infection, and timely recognition is essential to avoid unnecessary interventions. The constellation of endoscopy and imaging findings supported a diagnosis of GOO due to duodenal compression from retroperitoneal involvement. The patient underwent gastrostomy tube placement for decompression and was started on total parenteral nutrition due to oral intolerance. Eventually the patient was started on a prednisone taper with a plan to start long term Rituximab. This case illustrates an uncommon GI presentation of IgG4-RD manifesting as GOO
Figure: Image showing retroperitoneal fibrosis with distended stomach
Disclosures: Warsha Korani indicated no relevant financial relationships. Arham Siddiqui indicated no relevant financial relationships. Fatmaelzahraa Abdelfattah indicated no relevant financial relationships. Adel Farhoud indicated no relevant financial relationships.
Warsha Korani, MD1, Arham Siddiqui, 2, Fatmaelzahraa Abdelfattah, MD3, Adel Farhoud, MD4. P0893 - A Rare Case of IgG4-Related Disease Presenting as Gastric Outlet Obstruction in a Patient With Retroperitoneal Fibrosis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.