Faisal Mehmood, MD1, Hajra Jamil, MD2, Osama A. Faridi, 3, Joseph Fares, MD4 1HonorHealth, Glendale, AZ; 2Services Institute of Medical Sciences, Lahore, Pakistan, Glendale, AZ; 3Midwestern University, Tempe, AZ; 4HonorHealth, Phoenix, AZ Introduction: Russell body gastritis (RBG) is a rare gastrointestinal (GI) inflammatory condition characterized by the accumulation of plasma cells containing dense eosinophilic cytoplasmic inclusions, i.e., Russell bodies. It can be associated with both neoplastic and non-neoplastic conditions. We present a case of RBG in an elderly male who had dysphagia.
Case Description/
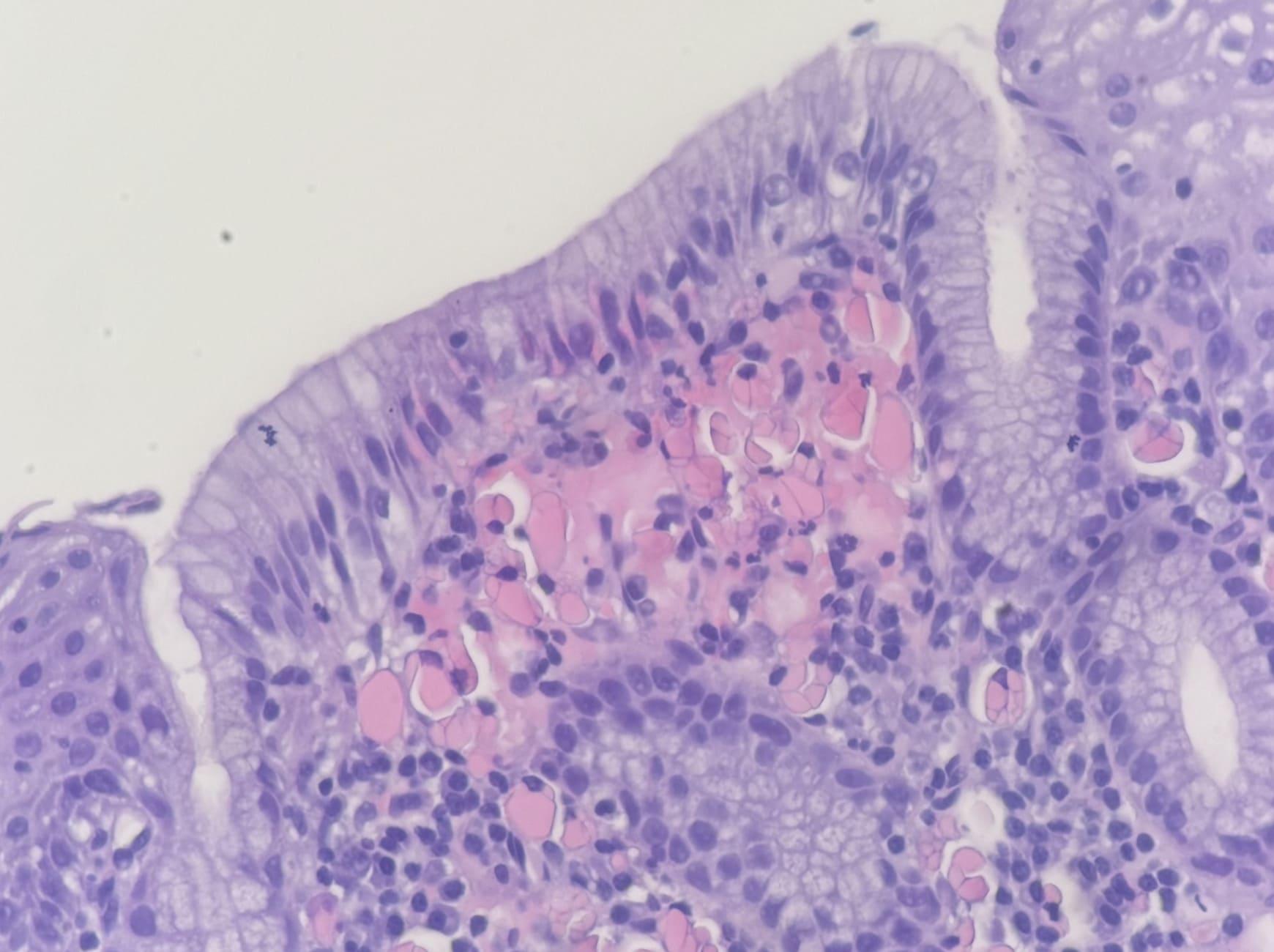
Methods: An 89-year-old male was admitted to the hospital for a mechanical fall. His past medical history was pertinent for aortic stenosis status post valve replacement, hypertension, hyperlipidemia, atrial fibrillation, and prostate cancer status post prostatectomy. Initial laboratory tests revealed a normal blood count, renal function, and liver function. Computed tomography (CT) scan of the entire body did not reveal any fractures or bleeding. He reported having dysphagia to solids for the last few months. He underwent an upper endoscopy and was found to have a small Zenker diverticulum, LA grade B esophagitis, and gastritis. Esophagus biopsies revealed plasma cells with distinctive eosinophilic inclusions (Mott cells) suggestive of RBG (Figure 1). Gastric biopsies showed chronic gastritis, and H. pylori was negative. CD138 immunohistochemistry revealed plasma cells. He underwent Zenker’s myotomy and had an uneventful hospital course. Discussion: RBG was first reported by Tazawa in a gastric biopsy in 1998. Since then, more than 40 cases of RBG have been reported, in addition to 7 cases of Russell body esophagitis. Stomach, especially antrum is the most common site affected by Russell body accumulation in the GI tract. However, these lesions can also be seen in duodenal heterotopic gastric mucosa, gastric cardia, and small and large intestine, including an unusual presentation of an inflammatory polyp in the colon. The pathogenesis of RBG can be multifactorial. It can cause dysphagia and is associated with infections like H. pylori, HIV, HCV, and candida esophagitis. H. pylori eradication usually results in clinical, endoscopic, and microscopic improvement in these patients. Various malignancies have been associated with this rare entity, including gastric adenocarcinoma, signet ring carcinoma, and gastric carcinoma associated with EBV. Differential diagnosis includes signet ring carcinoma, especially eosinophilic variant, hepatoid gastric carcinoma, epithelioid GI stromal tumor, plasma cell dyscrasias, and lymphoproliferative diseases, including lymphomas with signet ring cell morphology (e.g., follicular lymphoma).
Figure: The section shows gastroesophageal junctional mucosa with lamina propria expanded by chronic inflammation. A subset of plasma cells displays prominent intracytoplasmic eosinophilic globular inclusions ("mott-cell" morphology). No Helicobacter organisms are detected by routine stain or immunohistochemistry.
Disclosures: Faisal Mehmood indicated no relevant financial relationships. Hajra Jamil indicated no relevant financial relationships. Osama Faridi indicated no relevant financial relationships. Joseph Fares indicated no relevant financial relationships.
Faisal Mehmood, MD1, Hajra Jamil, MD2, Osama A. Faridi, 3, Joseph Fares, MD4. P0737 - Russell Body Gastroesophagitis: An Uncommon Histology With Common Symptoms, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.