Dharma Ayer, BS, Micheal Tadros, MD Albany Medical Center, Albany, NY Introduction: High-resolution manometry (HRM) is used to evaluate esophageal motor function and classify motility disorders via the Chicago Classification (CC). Although CC remains the standard diagnostic tool, it may have limitations in patients with surgically altered anatomy. We present a case of post-bariatric dysphagia where standard interpretation was inadequate due to altered foregut physiology and compartmentalization below the LES region, not included in CC criteria.
Case Description/
Methods: A 57-year-old female patient with a history of morbid obesity, who initially underwent gastric banding later converted to Roux-en-Y gastric bypass, presented with persistent dysphagia. Her surgical history was notable for multiple prior abdominal procedures and adhesiolysis for reccurent small bowel obstruction. Initial evaluation with upper endoscopy revealed a small hiatal hernia, an intact and widely patent gastrojejunal anastomosis, and no evidence of mechanical obstruction.
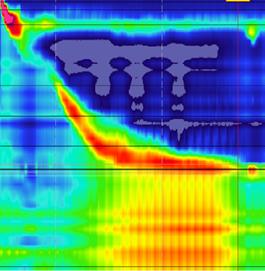
HRM was performed to evaluate for any motility disorder. The study revealed multiple high-pressure zones below the LES, with pressurization between the LES and distal pressure zones including the diaphragmatic hiatus (pressure inversion point or PIP). Impedance testing showed incomplete bolus clearance across all swallows. Provocative maneuvers, including apple viscous swallows and multiple rapid swallows, demonstrated similar findings.
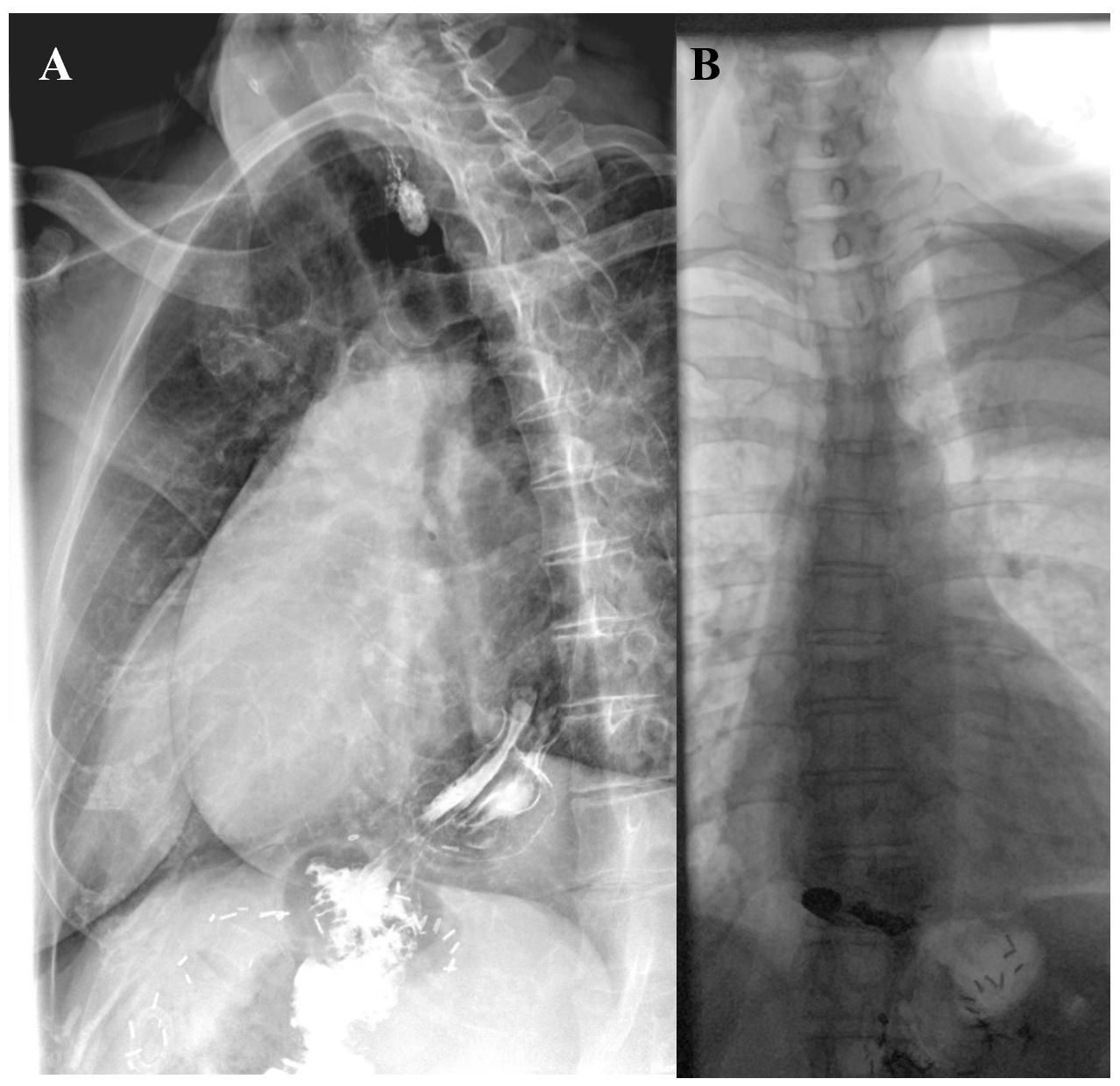
Subsequent barium esophagram demonstrated a hiatal hernia, with majority of the gastric pouch located above the diaphragm. Barium pill 13 mm swallow was retained at the level of the hiatus. The findings were interpreted as secondary to altered postsurgical anatomy and possible extrinsic compression at the level of the hiatus due to intra-abdominal scarring. Given her high operative risk, the patient underwent empiric dilation to 17 mm using a Savary dilator. At two-month follow-up, she reported partial improvement in dysphagia symptoms. Discussion: This case illustrates the importance of integrating HRM findings with a comprehensive clinical context. Although CC would not have categorized this study as pathologic in isolation, further evaluation revealed abnormal pressurization patterns below the LES likely due to herniation of the gastric pouch, altered surgical anatomy and adhesions. This highlights that HRM should not be interpreted solely within a diagnostic framework or classification, but in conjunction with a patient's history, imaging, and endoscopic findings to inform individualized management.
Figure: Figure 2: (A) Barium esophagram revealing hiatal hernia with gastric pouch partially above diaphragm. (B) Barium tablet (13 mm) retained at the level of the hiatus.
Disclosures: Dharma Ayer indicated no relevant financial relationships. Micheal Tadros indicated no relevant financial relationships.
Dharma Ayer, BS, Micheal Tadros, MD. P0720 - Limitations of the Chicago Classification in a Post-Gastric Bypass Patient With Pathology Below the LES, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")