Ria Ghose Kundu, MD, Jose Machain, MD HonorHealth, Scottsdale, AZ Introduction: Foreign body ingestion is rare in adults compared to children. In 95% of cases, it is accidental. While 80–90% of ingested foreign bodies pass spontaneously, 10–20% require endoscopic intervention. This case report aims to highlight a rare cause of dysphagia and suspected food bolus impaction: cervical spine hardware erosion into the pharynx, and to emphasize the importance of thorough history-taking, especially surgical history, in evaluating foreign body ingestion. The case demonstrates the role of multidisciplinary planning (GI, ENT, Anesthesia, Surgery) in managing complex upper GI endoscopy cases, and underscores the need to review prior imaging in high-risk patients before performing endoscopy.
Case Description/
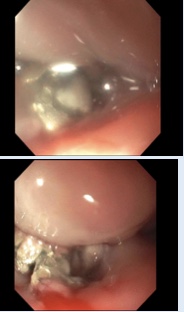
Methods: A 65-year-old female with COPD, CKD (Stage 2–3), RA, and tracheal stenosis presented with nausea, vomiting, and dysphagia after eating pizza on 09/09/24. She was unable to swallow liquids and developed inspiratory stridor. Upon ED arrival (~5:00 PM), her vital signs were HR 107, RR 16, BP 149/81, and SpO₂ 98%. The patient had a history of cervical spinal fusion (2003) with post-op airway distress, subsequent tracheostomy after failed extubation, and right vocal cord paresis that resolved. She had multiple intubations without further tracheostomies. The patient underwent EGD under general anesthesia the following day with ENT and anesthesia support. Fiberoptic nasotracheal intubation was successful via the right nostril. A pediatric endoscope was used after the adult scope failed to pass. Findings included cervical spine hardware eroding into the posterior pharynx/cricopharyngeus. No food bolus was visualized. Prior CT from 08/21/24 confirmed the same finding. The patient was extubated in the OR and made NPO. Spine surgery was consulted for hardware removal, and a G-tube was placed for feeding the following day Discussion: Suspected food bolus impaction can mask underlying anatomical causes of obstruction, such as cervical spine hardware erosion, which may present with similar symptoms. A detailed surgical history and review of prior imaging can prevent misdiagnosis and unnecessary, potentially risky procedures. Multidisciplinary coordination between GI, ENT, anesthesia, and surgery teams is crucial in managing high-risk airway cases. Endoscopic attempts without proper evaluation of patient history and prior imaging can lead to complications, underscoring the need for a comprehensive approach to foreign body ingestion cases.
Figure: EGD finding
Figure: CT scan neck
Disclosures: Ria Ghose Kundu indicated no relevant financial relationships. Jose Machain indicated no relevant financial relationships.
Ria Ghose Kundu, MD, Jose Machain, MD. P0719 - Cervical Spine Hardware Erosion: The Hidden Cause of Dysphagia That Mimics Food Obstruction, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")