Sadie De Silva, MD, Matthew Mishoe, DO, Dustin Kilpatrick, DO UNC Health Blue Ridge, Morganton, NC Introduction: Esophageal cancer is relatively rare and comprises 1.1% of all new cancer cases in the US population. Esophageal squamous cell carcinoma (ESCC) incidence has declined in the US over the past 20 years while esophageal adenocarcinoma has increased. The 5-year survival for all stages of esophageal cancer combined is around 20%. ESCC frequently presents at an advanced stage with the most common metastatic sites being lung, liver, and distant lymph nodes. Bone metastasis is rare but has been identified. Our case report highlights an unusual presentation of sacral metastasis from esophageal squamous cell carcinoma and discusses the management and clinical implications.
Case Description/
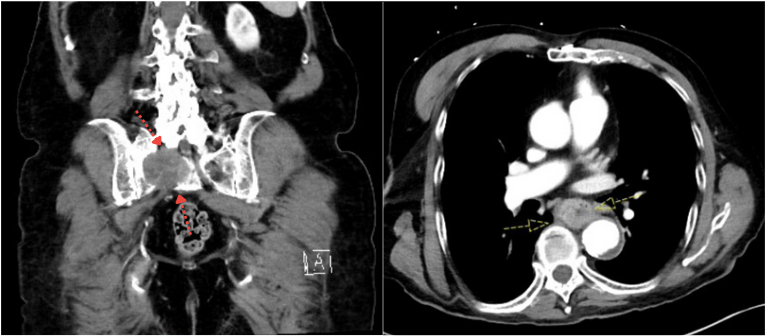
Methods: We present an 82 year-old male with past medical history of gastroesophageal reflux who presented to emergency with long-standing, progressive back pain over the past few months that radiated to the right hip and leg. Patient was admitted for intractable pain and CT L-spine revealed a new finding of 5.3 x 5.1 cm destructive lytic right sacral mass (Figure 1a). Patient then underwent IR-guided biopsy of sacral mass which was consistent with squamous cell carcinoma. To further ascertain primary source of squamous cell carcinoma, CT abdomen pelvis was ordered and showed circumferential thickening of distal esophagus with regional adenopathy (Figure 1b). Upon further questioning, patient reported a long-standing history of dysphagia to solids and nausea. Upper endoscopy showed a partial obstructing, partially circumferential mass in mid esophagus with stigmata of bleeding with biopsies consistent with squamous cell carcinoma (Figure 2). Patient was seen by oncology and started on 8 rounds of palliative radiation and remained hospitalized through due to intractable pain. Patient opted to transition to comfort care after 8th cycle of radiation and was discharged home with hospice. Discussion: Sacral metastasis from esophageal squamous cell carcinoma, while rare, is a recognized metastatic site of esophageal cancer. Esophageal cancer should be considered as part of the differential for primary site of sacral metastasis when diagnosis is unclear as long-standing gastrointestinal symptoms may be underreported as seen with our patient. Diagnosis is made by endoscopy and confirmed histologically and management is on a case by case basis, but is generally palliative with a focus on systemic therapy and symptom control.
Figure: Figure 1: a. CT of destructive lytic right sacral ala mass measuring 5.3 cm (red arrows); b. CT of circumferential wall thickening in mid to distal esophagus (yellow arrows) below the level of the carina measuring up to 3.5 cm with enlarged LNs adjacent to esophagus measuring up to 1.6 cm.
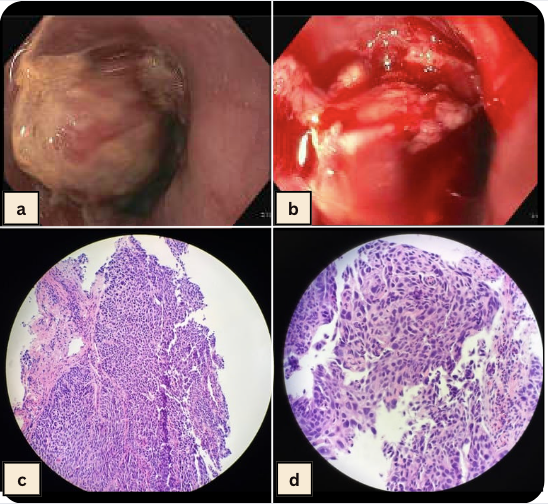
Figure: Figure 2: a, b. EGD of partially obstructing, partial circumferential mid-esophageal mass 4 cm in length, around 4 cm proximal to GEJ; c, d. Biopsy of esophageal mass: higher magnification of malignant squamous epithelium showing pleomorphic nuclei and numerous mitoses, infiltrating into the submucosa.
Disclosures: Sadie De Silva indicated no relevant financial relationships. Matthew Mishoe indicated no relevant financial relationships. Dustin Kilpatrick indicated no relevant financial relationships.
Sadie De Silva, MD, Matthew Mishoe, DO, Dustin Kilpatrick, DO. P0714 - A Man With Intractable Back Pain – A Rare Presentation of Metastatic Esophageal Squamous Cell Carcinoma, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.