Urmimala Chaudhuri, DO1, Omar Zayed, BS2, Hassan Zreik, MD2, Drew Triplett, DO2 1Wright State University, Centerville, OH; 2Wright State University Boonshoft School of Medicine, Dayton, OH Introduction: Zenker’s diverticulum (ZD) is an uncommon pharyngoesophageal outpouching that typically presents in older adults and presents with dysphagia and aspiration. Presentation before age 60 with primary respiratory symptoms is rare. We report a case of a large ZD causing near-complete esophageal obstruction and progressive respiratory distress. This case emphasizes the importance of early recognition, appropriate imaging, and multidisciplinary management.
Case Description/
Methods: 55-year old male initially presented with worsening shortness of breath. Gastroenterology (GI) was consulted after he reported several months of dysphagia to solids and liquids with an unintentional 25-pound weight loss. He underwent a videofluoroscopic swallow study which demonstrated significant oropharyngeal dysphagia. He was advised to follow a full liquid diet, however, symptoms still persisted. An esophagogastroduodenoscopy (EGD) revealed a severe upper esophageal stricture with complete obstruction and retained food material. This prompted barium esophagram study which revealed a large Zenker’s diverticulum causing near-complete obstruction of the upper thoracic esophagus. Neck computed tomography confirmed a diverticulum compressing the proximal esophagus. Otolaryngology (ENT) was consulted and he underwent rigid esophagoscopy with transcervical Zenker’s diverticulectomy. Postoperative esophagram showed no leak and his diet was advanced before discharge in stable condition. Discussion: Our case highlights that ZD can present in atypical ways. It can arise and manifest with primarily respiratory symptoms and nutritional decline secondary to mass effect. A stepwise diagnostic approach was crucial: the swallow study and barium esophagram identified the diverticulum and CT delineated its extent to guide surgical planning. If left untreated, a large ZD can lead to complications such as aspiration pneumonia, perforation with mediastinitis, or esophageal cancer. Management strategies depend on the size and anatomy of the diverticulum ranging from flexible endoscopic myotomy to open surgical diverticulectomy. Given these risks, early intervention is critical. In our case, the size and severity of the obstruction warranted a transcervical surgical approach to relieve the obstruction and prevent further morbidity. A multidisciplinary approach proved essential; collaboration between GI and ENT. Early identification and a multidisciplinary approach are critical for successful outcomes.
Figure: Figure 1. Barium esophagram showing large Zenker’s diverticulum causing near obstruction of the upper thoracic esophagus.
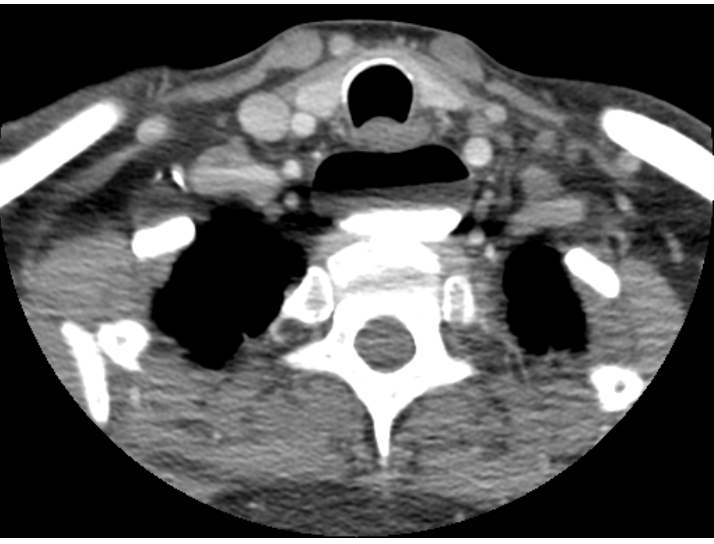
Figure: Figure 2. CT soft tissue neck showing large Zenker’s diverticulum with compression of the proximal esophagus.
Disclosures: Urmimala Chaudhuri indicated no relevant financial relationships. Omar Zayed indicated no relevant financial relationships. Hassan Zreik indicated no relevant financial relationships. Drew Triplett indicated no relevant financial relationships.
Urmimala Chaudhuri, DO1, Omar Zayed, BS2, Hassan Zreik, MD2, Drew Triplett, DO2. P0705 - A Chokehold in the Neck: Zenker’s Diverticulum With Complete Obstruction, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.