
Sunday Poster Session
Category: Endoscopy Video Forum
Paul Hong, MD
University of Chicago, NorthShore University Health Systems
Chicago, IL
Cholecystohepatic fistula is a rare complication resulting from a gallbladder disease such as an acute inflammation, perforation, or malignancy. EUS-GBD may be an effective strategy to manage this challenging complication.
Case Description/
Methods:
70-year-old female established with newly diagnosed gallbladder adenocarcinoma with extrahepatic biliary obstruction treated with ERCP and transpapillary biliary stenting experienced progression of disease, requiring surgical intervention to be aborted due to invasion into the right hepatic lobe. Patient underwent repeated intervention with plan to optimize for chemotherapy, including celiac plexus neurolysis and repeat ERCP for upsizing to metal biliary stenting when she endorsed new fevers and progressive failure to thrive.
On repeat imaging, she was found to have progressed invasion of her cancer as well as findings suggestive of gallbladder microperforation and cholecystohepatic fistula with developing liver abscess. After multi-disciplinary discussion and patient preference to avoid percutaneous drainage, she underwent EUS-gallbladder drainage for suppurative cholecystitis as well as EUS-gastroenterostomy to improve oral intake.
After two weeks (to allow for fistula maturation to the gallbladder) endoscopic access through the created cholecystoduodenostomy allowed for endoscopic extraction of over 50 gallstones that likely prevented drainage of the abscess. Next, drainage of the hepatic abscess was performed with a draining double pigtailed stent through the cholecystohepatic fistula. She tolerated the procedure well with improvement of her clinical status but ultimately decided to enter hospice care due to grim oncologic prognosis and later died, several weeks after abscess drainage without fever recurrence.
Discussion:
An effective treatment for suppurative cholecystitis with malignant cholecystohepatic fistula resulting in liver abscess involved a staged approach utilizing EUS-gallbladder drainage followed by endoscopic drainage of the liver abscess through the cholecystohepatic fistula. While EUS-GBD has been shown to be a safe and effective modality compared to a percutaneous route of drainage in non-surgical candidates with acute cholecystitis, this case demonstrates that a hepatic abscess drainage was also possible through the same channel.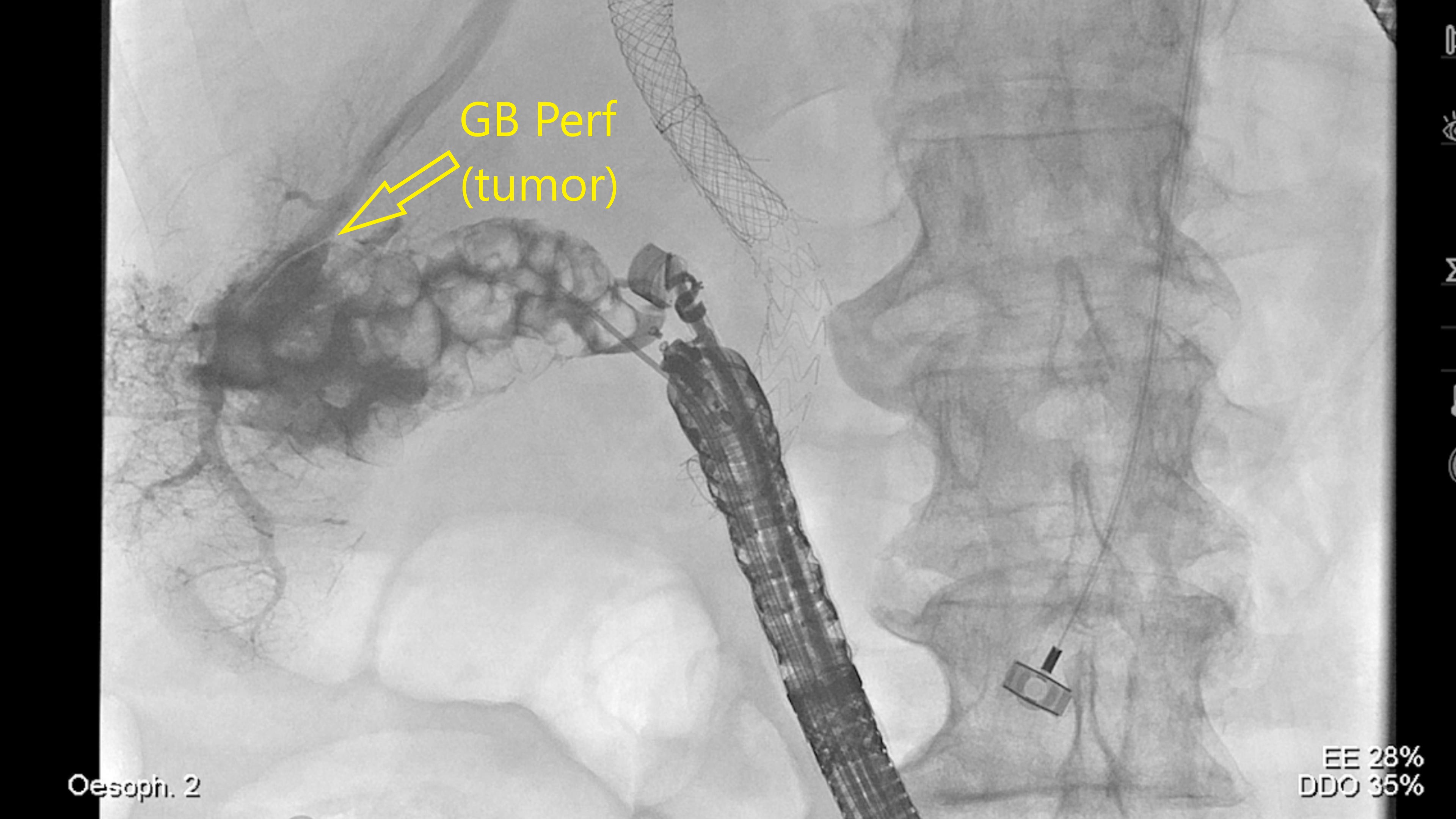
Figure: Figure 1: Gallbladder with microperforation and cholecystohepatic fistula. 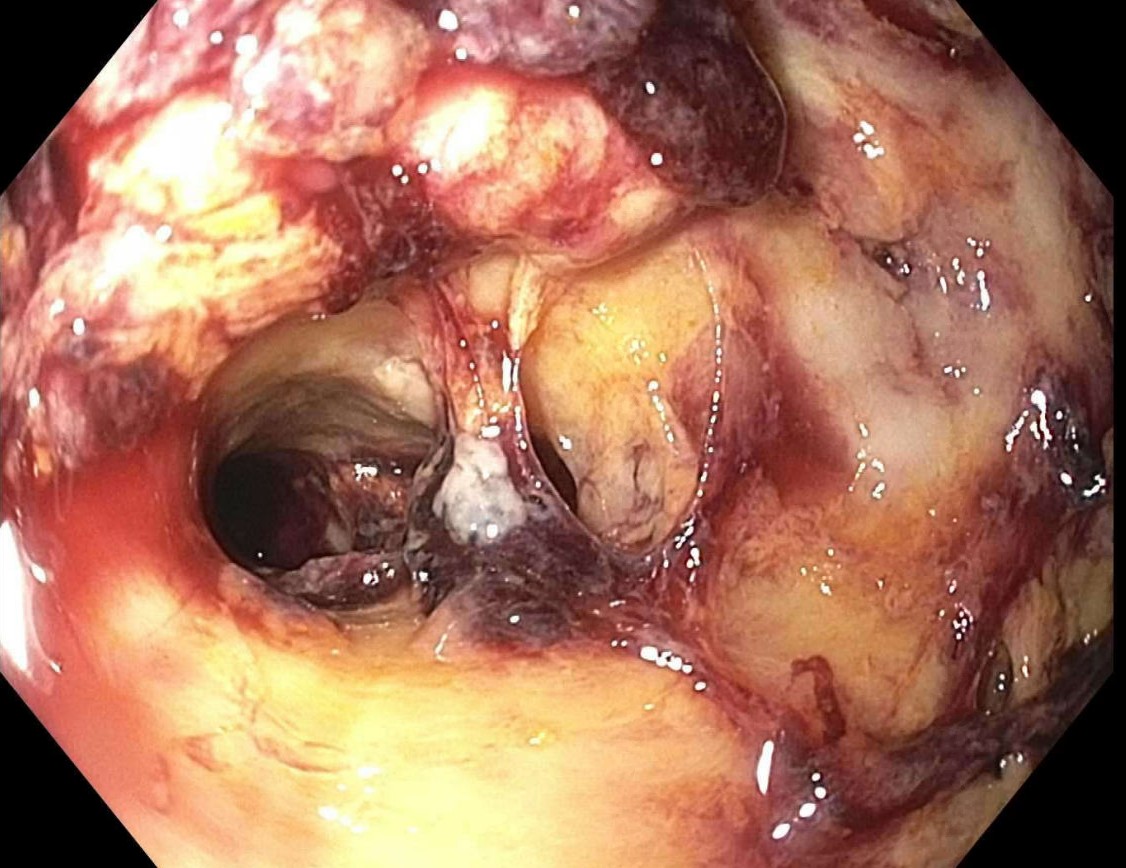
Figure: Figure 2: Cholecystohepatic fistula.
Disclosures:
Paul Hong indicated no relevant financial relationships.
Edward Villa: Olympus Corporation – Consultant.
Paul Hong, MD1, Edward C. Villa, MD2. P0583 - Endopalliation in Patient With Metastatic Gallbladder Carcinoma With Biliary and Gallbladder Obstruction, Failure to Thrive, and Hepatic Abscess in Setting of Malignant Cholecystohepatic Fistula, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.