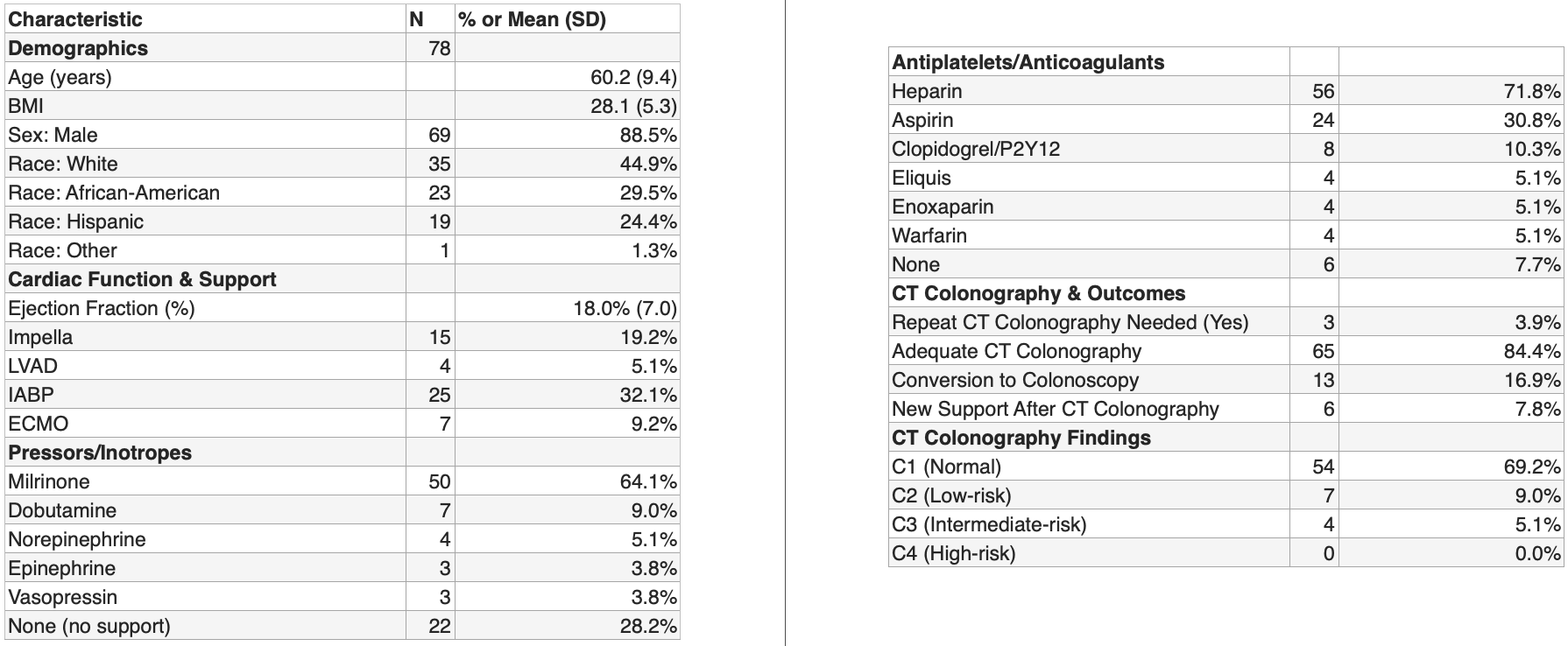
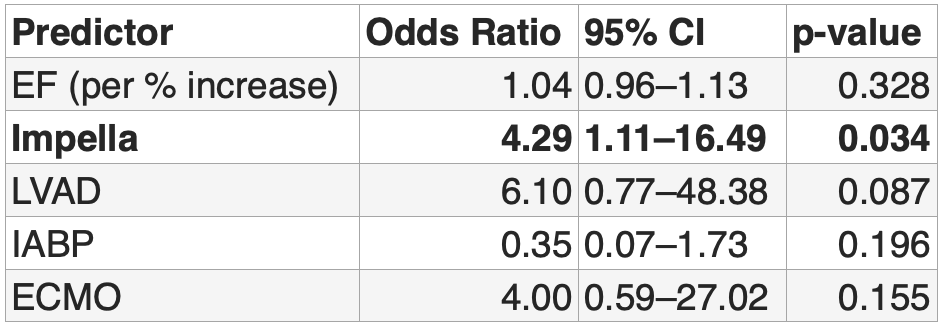
Zaid Ansari, MD, Akram Ahmad, MD, Osama Sherjeel Khan, MD, Tasneem Jamal Al-Din, MD, Fernando Castro, MD Cleveland Clinic Florida, Weston, FL Introduction: Patients undergoing evaluation for orthotopic heart transplantation (OHT) often exhibit compromised hemodynamics, frequent use of mechanical circulatory support, and a high burden of anticoagulation, all of which complicate colorectal cancer (CRC) screening. Colonoscopy, while standard, carries significant procedural risks in this population. CT Colonography (CTC) presents a less invasive alternative, but limited data exist regarding its safety and diagnostic performance in pre-OHT candidates. Methods: This retrospective cohort study evaluated 78 patients in Cleveland Clinic who underwent CTC during OHT evaluation at a single tertiary center. We analyzed demographic characteristics, cardiac function, advanced mechanical support modalities (e.g., Impella, LVAD, ECMO, IABP), anticoagulation profiles, and CRC related patient history. Primary and secondary endpoints included the adequacy of CTC studies, rate of conversion to colonoscopy, and incidence of hemodynamic deterioration necessitating additional support post-CTC. Results: Our cohort had a mean age of 60.2 years (SD ±9.4) and was predominantly male (88.5%). This cohort had a mean ejection fraction of 18.0% (SD ±7.0). Mechanical support devices were used in 65% of patients, and 72% required use of vasopressors or inotropes. Systemic anticoagulation or antiplatelet therapy at the time of CTC was noted in 92% of the study population. CTC was technically adequate in 84.4% of patients. A subsequent colonoscopy was performed in 13 patients (16.9%), primarily due to suboptimal bowel preparation or indeterminate findings. Some of these patients could have potentially undergone repeat CTC with additional preparation. The only statistically significant predictor of colonoscopy after CTC was the presence of Impella support (OR 4.29, 95% CI 1.11–16.49, p = 0.034). For the 24 hours after CTC, new or escalated hemodynamic support was required in 8% of patients and no major complications were reported. During a mean follow-up period of 16.2 months, no cases of CRC or advanced adenoma were diagnosed among those with follow up in GI clinic. Discussion: CT colonography demonstrates potential as a safe and effective CRC screening modality in high-risk OHT candidates. It is technically feasible in most patients with a low rate of conversion to colonoscopy and minimal adverse clinical events. Importantly, no patient experienced clinically significant deterioration attributable to the CTC procedure, providing its safety in pre-heart transplant workup.
Figure: Table 1: Baseline Characteristics
Figure: Table 2: Predictors Of Conversion To Colonoscopy
Disclosures: Zaid Ansari indicated no relevant financial relationships. Akram Ahmad indicated no relevant financial relationships. Osama Sherjeel Khan indicated no relevant financial relationships. Tasneem Jamal Al-Din indicated no relevant financial relationships. Fernando Castro indicated no relevant financial relationships.
Zaid Ansari, MD, Akram Ahmad, MD, Osama Sherjeel Khan, MD, Tasneem Jamal Al-Din, MD, Fernando Castro, MD. P0518 - Safety and Adequacy of CT Colonography for Colorectal Cancer Screening in Pre-Heart Transplant Evaluation, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.