University of Puerto Rico School of Medicine Caguas, PR
VIctor J. Colon Sanchez, BS1, Andres I. Colon Sanchez, BS, BA1, Victor Colon Vazquez, MD, FACG2 1University of Puerto Rico School of Medicine, Caguas, Puerto Rico; 2Instituto Digestivo De Puerto Rico, PSC, Caguas, Puerto Rico Introduction: Chilaiditi’s sign is a rare radiologic finding of unknown etiology that involves interposition of the colon between the liver and the right hemidiaphragm. When symptomatic, it is called Chilaiditi’s syndrome. It can present with mild non-specific symptoms to severe manifestations necessitating prompt diagnosis and management. There is a potential association with pulmonary and gastrointestinal malignancies. Cases reported in the literature have follow-ups of only a few months. We present the first case report with a seven-year follow up and showing long-term symptoms resolution without surgical intervention.
Case Description/
Methods: A 56 y/o man presented with a 6-week history of right upper quadrant (RUQ) abdominal (abd) pain described as low intensity, constant, with episodes of severe intensity lasting 1-2 hours, associated with bloating, heartburn, constipation and abd distention that improved with regular bowel movements. The patient has consulted several physicians, had multiple labs and x-ray studies, a colonoscopy within a year, without revealing a diagnosis. The physical exam findings were normal except for RUQ and epigastric mild abd tenderness without distention, guarding or rebound. Due to a family history of gastric cancer and an uncertain etiology of the abd pain, an EGD and a contrast CT scan of the abd/pelvis were done. The EGD revealed a small hiatal hernia. The CT scan revealed colonic interposition between the liver and an elevated right hemidiaphragm (see figures 1 and 2) consistent with Chilaiditi’s sign. These findings, initially overlooked, were identified while reviewing the CT scan images. The radiologist was made aware of the findings and issued an amended report. The differential diagnoses excluded were peptic ulcer disease, gastric malignancy, gallbladder disease, vascular and urologic causes, appendicitis and colon cancer. There was an excellent response to conservative management consisting of simethicone, stool softeners, osmotic laxatives, exercise, and high fiber diet. Patient has remained symptom free for 7 years on this conservative regimen. Discussion: This is the first documented case of Chilaiditi’s syndrome with long term follow-up. It highlights the diagnostic challenge posed by this condition, the need for clinicians’ awareness when evaluating patients with RUQ abd pain, the importance of reviewing radiologic images, and supports the evidence of conservative management as the mainstay of therapy.
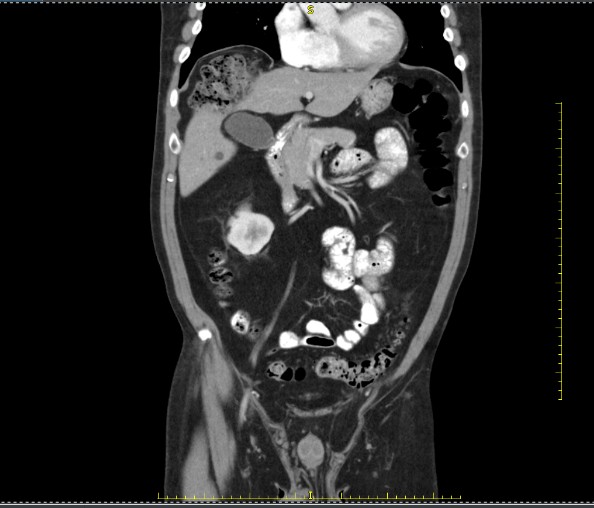
Figure: Figure 1 – Chilaiditi’s sign: CT scan Coronal view with colon having air and stool interposed between the liver and the elevated right diaphragm.
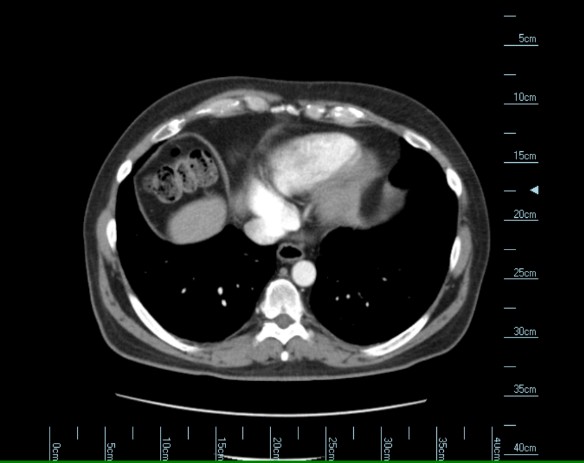
Figure: Figure 2 – Chilaiditi’s sign: CT scan Axial image with colon interposition just under the right diaphragm and anterior to the liver superior tip.
Disclosures: VIctor J. Colon Sanchez indicated no relevant financial relationships. Andres I. Colon Sanchez indicated no relevant financial relationships. Victor Colon Vazquez indicated no relevant financial relationships.
VIctor J. Colon Sanchez, BS1, Andres I. Colon Sanchez, BS, BA1, Victor Colon Vazquez, MD, FACG2. P0461 - Chilaiditi’s Syndrome: A Case Report of Conservative Management with a Seven-Year Follow-Up and Review of the Literature, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.