Mount Sinai South Nassau,Icahn School of Medicine at Mount Sinai Oceanside, NY
Rahul Anand, DO, MBBS1, Lenura Ziyadin, DO2, Muhddesa Lakhana, DO2, Dong Jun Yun, MD1, Jonathan Reyes, MD2, Kazim Kazbay, MD1 1Mount Sinai South Nassau, Oceanside, NY; 2Mount Sinai South Nassau,Icahn School of Medicine at Mount Sinai, Oceanside, NY Introduction: Adult intussusception is a rare clinical entity. Unlike pediatric intussusception, adult cases are typically secondary to an underlying pathologic lesion, with malignancy being the leading cause in colonic intussusception. Infectious etiologies, represent an important subset. We present two adult cases of intussusception and discuss the importance of endoscopic evaluation.
Case Description/
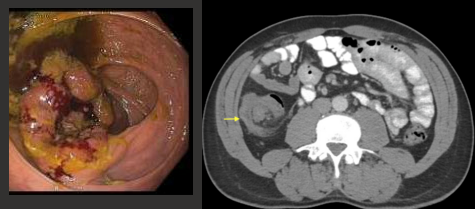
Methods: Case 1: 50-year-old male with no past medical history presented to the emergency department with a 4-month history of progressive left lower quadrant abdominal pain. Initially intermittent, the pain had become constant over recent weeks without associated gastrointestinal symptoms. CT abdomen/pelvis demonstrated ileocecal intussusception. Subsequent colonoscopy revealed a large 80mm x 50mm polypoid, infiltrative lesion at the ileocecal valve with partial luminal occlusion. Histopathologic analysis confirmed moderately differentiated adenocarcinoma. Patient underwent right hemicolectomy and adjuvant chemotherapy.
Case 2: A 30-year-old male presented with 3-day acute abdominal pain and watery diarrhea. CT showed pancolitis with hepatic flexure intussusception. HIV testing was negative. Stool studies revealed Salmonella. Colonoscopy successfully reduced the intussusception with water/air insufflation. Biopsy results showed colonic mucosa with chronic active colitis with cryptitis and crypt abscess formation. Patient was advised to follow up but was lost to follow up.
Discussion: Adult intussusception differs fundamentally from pediatric cases, requiring comprehensive evaluation for underlying pathology. While malignancy is the most common cause, infectious etiologies—including opportunistic infections in HIV patients (Kaposi's sarcoma, CMV colitis, lymphoma)—must be considered. Unlike pediatric management with pneumatic reduction, adult cases additionally mandates cancer screening and infectious workup, including HIV testing when appropriate.
Conclusion: These cases illustrate the diagnostic spectrum of adult intussusception. They underscore the critical importance of maintaining a high index of suspicion and broad differential when adult intussusception is identified. Urgent colonoscopy and cross-sectional imaging are essential to exclude malignancy. Early recognition enables optimal outcomes through timely surgical intervention or targeted medical therapy.
Figure: Case 1: Malignant appearing polypoid lesion at the ileocecal valve. CT abdomen/ pelvis axial view showing characteristic "target" sign.
Figure: Case 2 :Colonoscopy image capturing focal erythema and erosions after reduction of the intussusception. CT abdomen/pelvis cross sectional and coronal view showing intussusception at the hepatic flexure.
Disclosures: Rahul Anand indicated no relevant financial relationships. Lenura Ziyadin indicated no relevant financial relationships. Muhddesa Lakhana indicated no relevant financial relationships. Dong Jun Yun indicated no relevant financial relationships. Jonathan Reyes indicated no relevant financial relationships. Kazim Kazbay indicated no relevant financial relationships.
Rahul Anand, DO, MBBS1, Lenura Ziyadin, DO2, Muhddesa Lakhana, DO2, Dong Jun Yun, MD1, Jonathan Reyes, MD2, Kazim Kazbay, MD1. P0434 - Adult Intussusception: Two Cases Highlighting Diverse Etiologies and Management Approaches, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.