Tarah Magloire, MD1, Alexander J. Kaye, MD2, Ramez M.. Ibrahim, MD2, Tamta Chkhikvadze, MD1, Sushil K. Ahlawat, MD1 1SUNY Downstate Medical Center, Brooklyn, NY; 2SUNY Downstate Health Sciences University, Brooklyn, NY Introduction: Mycophenolate mofetil (MMF) is an inosine monophosphate inhibitor that selectively suppresses lymphocyte proliferation and is thus widely used in transplant medicine to prevent graft rejection. Gastrointestinal side effects are amongst the most reported, with several published cases of colitis as well as esophagitis. We present one of the first documented biopsy-proven cases of multiple concurrent colonic strictures developed in the setting of chronic MMF use.
Case Description/
Methods: A 60-year-old female with end-stage renal disease status post 3 dead-donor-renal transplants, on immunosuppressive regimen of 250 mg of MMF twice daily, who presented with 3 days of generalized abdominal pain, nausea, vomiting, and 2 days of severe constipation. She was noted with a distended, diffusely tender abdomen. Digital rectal exam showed no evidence of melena or hematochezia. The patient underwent CT abdomen/pelvis demonstrating multiple loops of dilated large and small bowel as well as 2 transition points in the descending colon with adjacent inflammatory changes and wall thickening.
The partial large bowel obstruction was initially thought to be secondary to large stool burden given a lack of clear mass on CTAP and evidence of previous stool burden on imaging in January 2024. EGD-colonoscopy was done and showed evidence of two colonic strictures; biopsies demonstrated crypt loss, lamina propria inflammation, and increased apoptotic bodies: findings consistent with chronic colitis and MMF-induced injury.
MMF was held, and medical decompression was initiated with improvement. She subsequently underwent therapeutic colonoscopy: the first colonic stricture was encountered at 15-20 cm from the anal verge and a second stricture at 30-35 cm from the anal verge; both inflammatory appearing, with no malignant features, and traversable with a pediatric colonoscope. Balloon dilation of both strictures was performed successfully to 12-15 mm. Discussion: Recurrent gastrointestinal symptoms in the setting of MMF use should raise suspicion for medication induced side effects. While esophageal strictures and colitis have been reported up to 10 years after initiation of MMF, few cases of colonic obstruction have been published. Management typically includes discontinuation or dose reduction, though this can be difficult in transplant patients with high immunologic risk. Our highly sensitized patient was switched to lower-dose enteric-coated mycophenolate sodium and scheduled for sequential colonic dilatations.
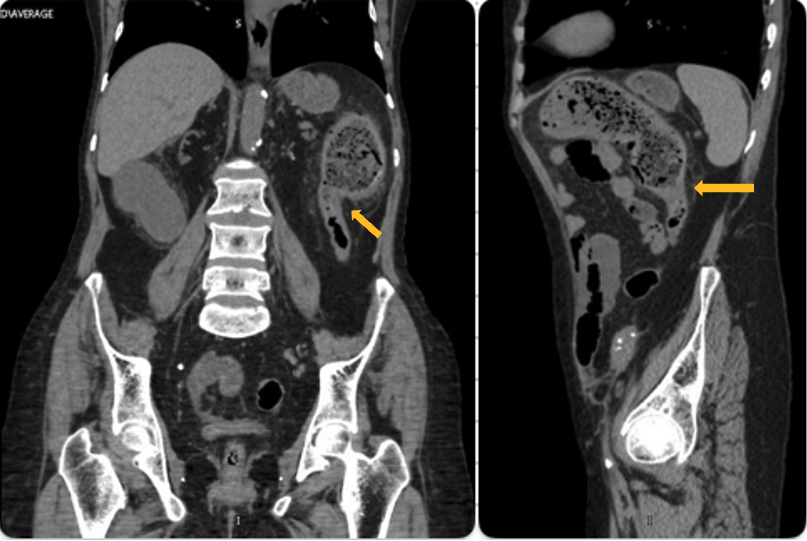
Figure: Coronal (left) and sagittal (right) views of descending colon stricture.
Figure: Colonic stricture seen on colonoscopy prior to dilation (left) and stricture seen through balloon dilator (right)
Disclosures: Tarah Magloire indicated no relevant financial relationships. Alexander Kaye indicated no relevant financial relationships. Ramez Ibrahim indicated no relevant financial relationships. Tamta Chkhikvadze indicated no relevant financial relationships. Sushil Ahlawat indicated no relevant financial relationships.
Tarah Magloire, MD1, Alexander J. Kaye, MD2, Ramez M.. Ibrahim, MD2, Tamta Chkhikvadze, MD1, Sushil K. Ahlawat, MD1. P0386 - Mycophenolate-Induced Multifocal Colonic Strictures: A Rare Presentation of Drug-Associated Colitis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")