
Sunday Poster Session
Category: Colon

Toni Chandler, MD
Robert Wood Johnson Medical School, Rutgers University
New Brunswick, NJ
Colonic lipomas are benign tumors composed of adipose tissue that are predominantly incidentally found, asymptomatic, less than 2 cm in diameter and do not require any treatment. Giant colonic lipomas, defined as greater than 4 cm are rare and can present with obstructive symptoms with treatment typically being endoscopic or surgical intervention depending on the size and location.
We present a rare case of autoamputation of a giant colonic lipoma in a patient with obstructive like symptoms prior to endoscopic intervention.
Case Description/
Methods:
A 40 year old female presented to GI clinic for one month history of intermittent left lower quadrant abdominal pain associated with bloating, diarrhea and rectal bleeding. Workup included an abdominal enhanced computer tomography (CT) which noted a 7.5 cm long and 3.9 x 3.8 cm cross sectional, longitudinally oriented, encapsulated, fat density intraluminal mass at the mid-descending colon: suspicious for a mucosal or submucosal lipoma. Subsequent colonoscopy confirmed a large descending colon lipoma extending through the lumen with an ulcerated tip. Biopsies were negative for malignancy. She was referred to advanced GI for endoscopic mucosal resection of the mass. One week prior to her scheduled colonoscopy, the patient had sudden onset of fecal urgency with spontaneous expulsion of the mass from the rectum into two separate pieces (Figure 1A and 1B) along with some blood. Following expulsion of the mass she reported feeling well with resolution of symptoms and no further subsequent blood in the stool. On repeat colonoscopy, a nodule was found near the splenic flexure with the surface appearing ulcerated but healing (Figure 1C). This was thought to be the attachment site of the giant lipoma. Biopsies were taken which came back as normal colonic mucosa with reactive changes. The patient continues to do well with no recurrence of her symptoms.
Discussion:
To our knowledge, this case highlights a rare situation of autoamputation and spontaneous expulsion of a giant colonic lipoma with approximately 15 cases reported worldwide. The underlying mechanism behind autoamputation remains unclear, however a suspected cause is tension or torsion from the lipoma twisting on itself causing ischemic necrosis.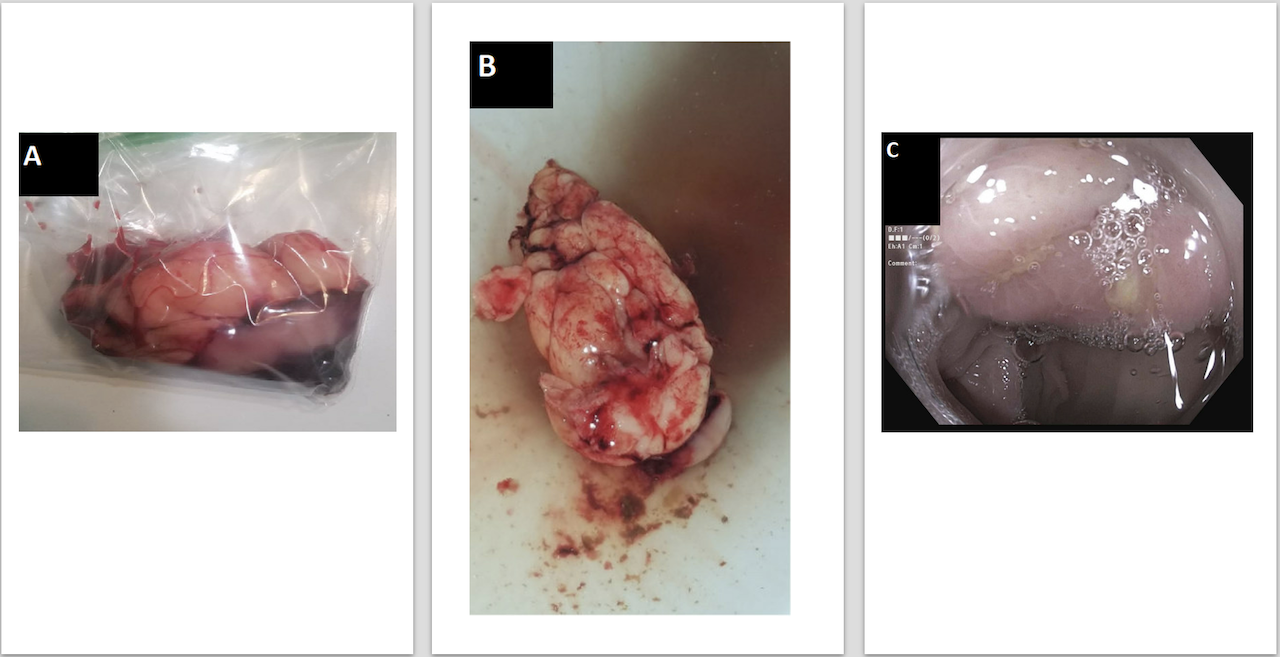
Figure: Figure 1. A and B. Pieces of the giant colonic lipoma after spontaneous self-expulsion. C. Inflammatory mound at splenic flexure where prior giant lipoma was located.
Disclosures:
Toni-Marie Chandler indicated no relevant financial relationships.
Petros Benias: Aurora Medical Technologies – CMO, Co-Founder. Boston Scientific – Consultant. Micro-tech Endoscopy – Consultant.
Toni-Marie Chandler, MD1, Petros Benias, MD2. P0352 - A Rare Case of Autoamputation and Spontaneous Expulsion of a Giant Colonic Lipoma, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.