
Sunday Poster Session
Category: Colon
 photo")
Sunny Kumar, MD (he/him/his)
Wright Center for Graduate Medical Education
Scranton, PA
Cylindrical battery ingestion is a rare but potentially serious occurrence that poses risks of mucosal injury, obstruction, or perforation due to chemical leakage or mechanical effects. Prompt identification and management are critical to prevent complications. Evidence-based guidelines emphasize observation and imaging for cylindrical batteries that have passed beyond the esophagus, with Intervention reserved for specific indications such as obstruction or prolonged retention. Here, we present a unique case of multiple AA and AAA battery ingestion, managed conservatively.
Case Description/
Methods:
A 34-year-old male with a history of bipolar disorder, polysubstance use, seizure disorder, GERD, and ventral hernia repairs (2016, 2017) presented after ingesting multiple AA and AAA batteries due to impulsivity over denial of reading materials. He reported mild epigastric pain and intermittent nausea but no emesis, heartburn, or changes in bowel habits. Denied suicidal ideations. Has prior ingestion of 2 batteries with self-resolution. On examination, he was comfortable with stable vitals. Bloodwork was unremarkable. Abdominal radiography revealed 8-9 cylindrical batteries likely in the distal stomach. A CT scan with intravenous contrast confirmed gastric location, intact bowel integrity, and absence of strictures or resections (Figure 1 A-B). Management included close monitoring for complications with serial imaging and administered a clear liquid diet with prokinetics. Erythromycin (250 mg TID) and Lactulose (45 mL TID) were given to promote bowel motility. The patient was closely monitored for signs of perforation, obstruction, or delayed passage. Serial X-rays revealed the progression of batteries into various parts of the colon and rectum, with the eventual complete passage of all batteries between Days 3 and 5 of hospitalization (Figure 2).
Discussion:
Cylindrical batteries pose mechanical and chemical hazards, especially in cases of prolonged retention or mucosal compromise. Management strategies vary depending on the battery's location and patient presentation. Evidence suggests that batteries beyond the esophagus can often be managed conservatively. In this case, the decision to avoid immediate intervention aligned with guidelines advocating for close monitoring and imaging to confirm passage into the small intestine or colon. Literature highlights the importance of individualized care, with surgery or endoscopic retrieval reserved for cases of failed progression or severe complications.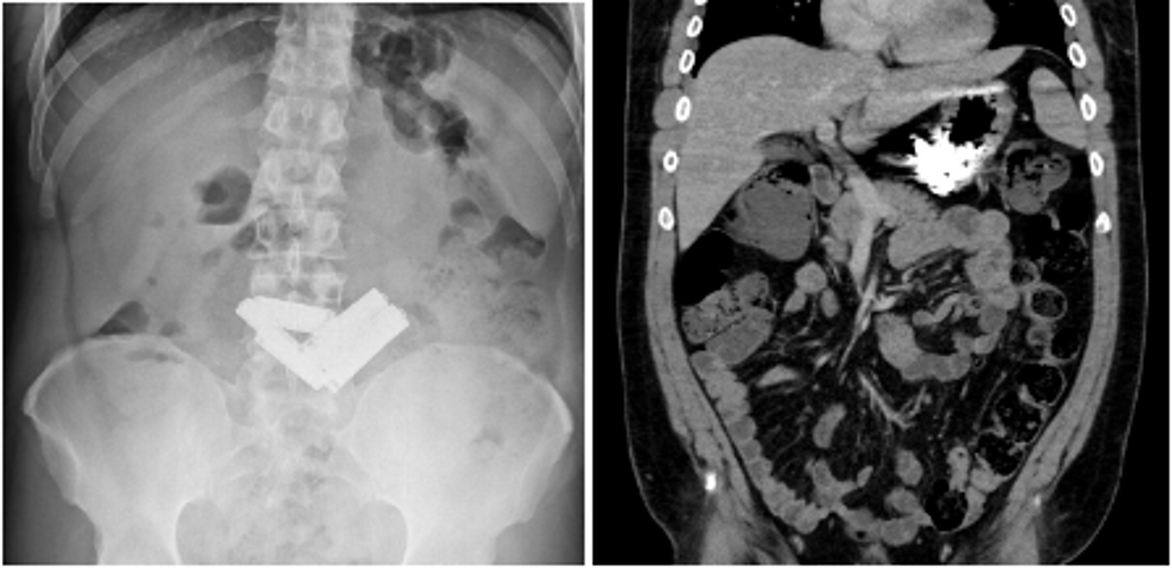
Figure: Figure 1- Abdominal X-Ray (A) and CT scan Abdomen (B) showing ingested batteries in the stomach and confirming distal intestinal integrity.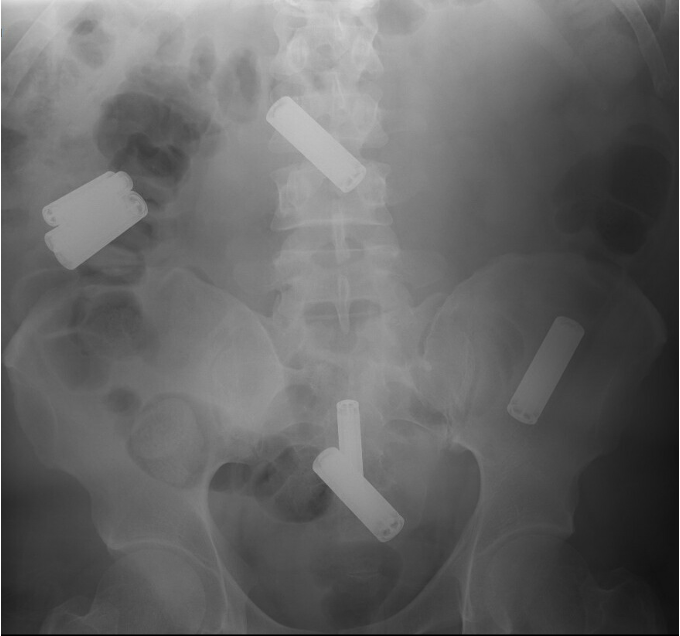
Figure: Figure 2 - Abdominal X-ray taken on 3rd day showing progression of ingested batteries.
Disclosures:
Sunny Kumar indicated no relevant financial relationships.
Ashok Kumar indicated no relevant financial relationships.
Avinash Nankani indicated no relevant financial relationships.
Rahul Kumar indicated no relevant financial relationships.
Fnu Aakash indicated no relevant financial relationships.
Archit Garg indicated no relevant financial relationships.
Muhammad Sohaib Alvi indicated no relevant financial relationships.
Udit Asija indicated no relevant financial relationships.
Sunny Kumar, MD1, Ashok Kumar, MD2, Avinash Nankani, MBBS3, Rahul Kumar, MD4, Fnu Aakash, MD5, Archit Garg, MD6, Muhammad Sohaib Alvi, MBBS, MD2, Udit Asija, MD7. P0339 - Charging Through: A Curious Case of Gastric Battery Ingestion, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.