
Sunday Poster Session
Category: Colon

Mohamed Eldesouki, MD
Saint Michael's Medical Center, New York Medical College
Newark, NJ
Lynch syndrome (LS) is the most common hereditary colorectal cancer (CRC) syndrome. Recent studies have shown that over time sporadic CRC has developed at younger ages. Whether the same trend is seen in patients with LS is not known. We aimed to compare the age distribution of new CRC diagnoses over time in patients with LS to that of the general population.
Methods:
We queried the TriNetX Network to examine adults (≥18 years) at risk for CRC at two-time intervals (2010-2017 and 2018-2024). Patients were stratified into two cohorts: those with hereditary GI cancer syndromes, including LS (ICD-10: Z15.09, Z14.8), and those without, representing the average-risk population. We excluded those at high-risk for CRC (familial adenomatous polyposis, benign neoplasm of the colon, Crohn’s disease, and ulcerative colitis). The endpoint was the distribution of CRC diagnoses across predefined age groups in patients with LS and the general population over time.
Results:
Between 2010 and 2024, 136,394 patients with LS and 106,114,751 at-risk individuals in the average population were identified. During 2010–2017, CRC diagnoses among LS patients mostly occurred between ages 45–54, while in the average-risk population, the peak was between 55–64 years. By 2018–2024, the peak age shifted earlier in both groups: 35–44 years in LS and 45–54 years in the average-risk cohort. The mean age of CRC diagnosis in patients with LS was 47±18 years, compared to 58±14 years in average risk patients through 2018-2024. Notably, 35% of CRC cases in LS patients occurred by age 44 in 2010–2017, compared to 51% in 2018–2024. Similarly, in the average-risk group, 34% of CRC cases occurred by age 54 in 2010–2017, rising to 41% in 2018–2024. CRC diagnoses after age 75 were rare among LS patients.
Discussion:
There has been a noticeable shift toward earlier onset of colorectal cancer in patients with Lynch syndrome over time similar to average-risk individuals. This shift might be attributed to environmental exposures, lifestyle patterns influencing cancer risk, or increased genetic testing with earlier initiation of colonic surveillance. A limitation of our study is that the ICD-10 codes used in our analysis lack specificity and may include other hereditary GI cancer syndromes. However, since LS makes up the majority of young-onset CRC, this may underestimate estimates, but the codes need further validation. Our findings imply that earlier screening in high-risk populations, such as those with LS, is warranted.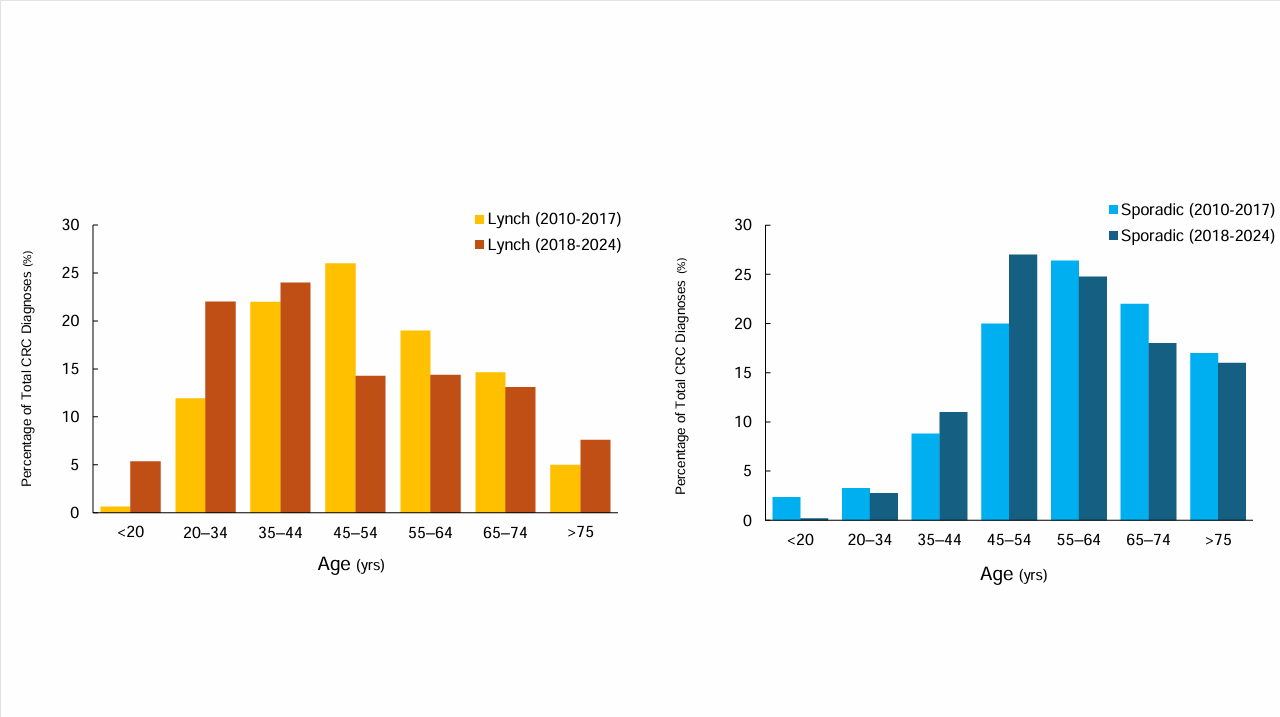
Figure: Figure 1. Age Distribution of Colorectal Cancer (CRC) Diagnoses in Lynch Syndrome and Sporadic Cases during 2010–2017 and 2018–2024.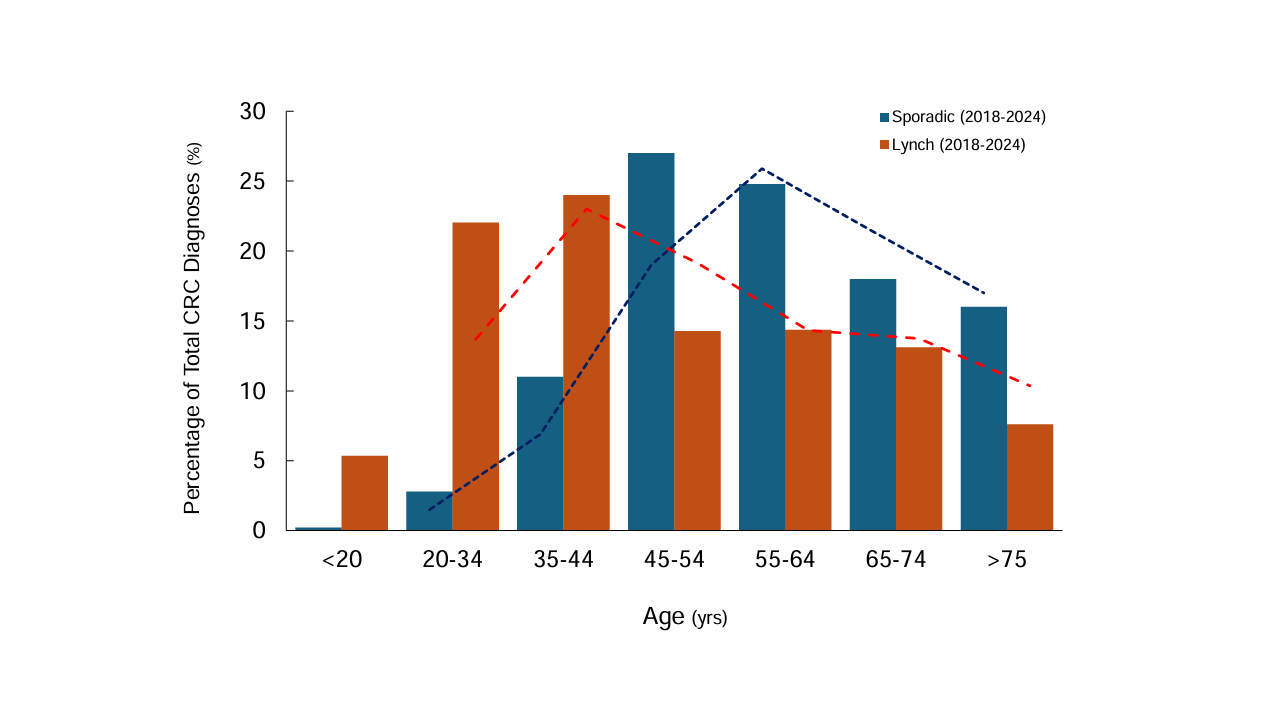
Figure: Figure 2. Temporal Shift in Age Distribution of CRC Diagnoses in Lynch Syndrome vs Sporadic Cases (2018–2024).
Disclosures:
Mohamed Eldesouki indicated no relevant financial relationships.
Ahmed Ibrahim indicated no relevant financial relationships.
Bryson Katona: Immunovia – Advisor or Review Panel Member, Consultant.
Carol Burke indicated no relevant financial relationships.
Aasma Shaukat: Freenome inc – Consultant.
Mohamed Eldesouki, MD1, Ahmed Ibrahim, MD2, Bryson W. Katona, 3, Carol Burke, MD, MACG4, Aasma Shaukat, MD, MPH, FACG5. P0273 - Parallel Younger Age Distribution Shifts in Lynch Syndrome and Sporadic Colorectal Cancer: A Nationwide Analysis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.