University of Texas Health San Antonio San Antonio, TX
Award: ACG Presidential Poster Award
Parth Patel, MD, MBA1, Shree Patel, MD1, Saatchi Kuwelker, MD1, Sherif Ibrahim, MD2, Sandeep Patel, DO1 1University of Texas Health San Antonio, San Antonio, TX; 2University of South Carolina School of Medicine, San Antonio, TX Introduction: Situs inversus totalis (SIT) is a congenital pathology in which thoracic and abdominal organs are transposed across the sagittal plane. Patients with SIT are often asymptomatic due to the maintained relationship between organs with most patients diagnosed incidentally on imaging for an unrelated illness. No definitive treatment has been identified due to the surgical complexity of rearranging all the transposed organs. In this case, we present a patient with recurrent pancreatitis presumed in the setting of SIT.
Case Description/
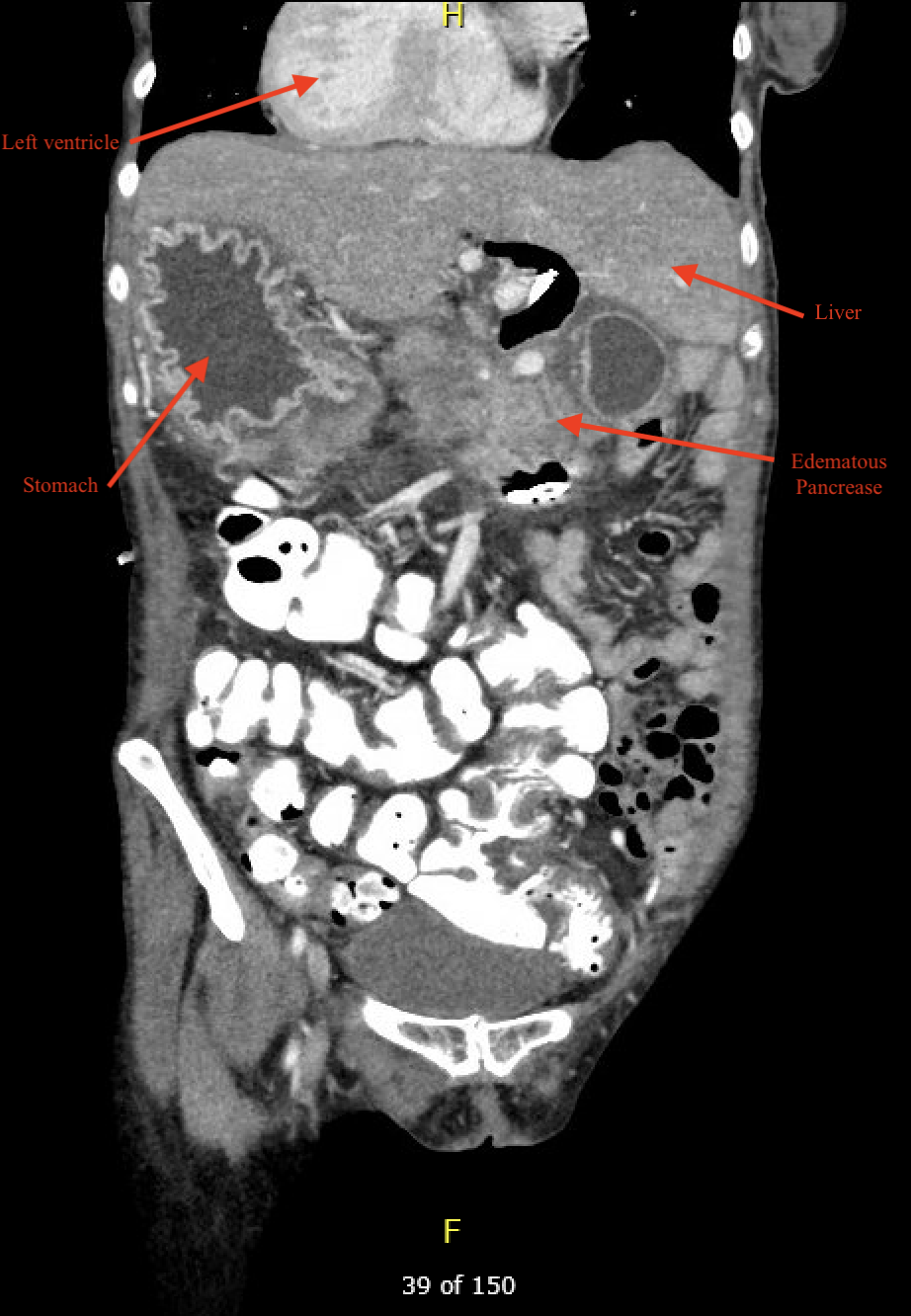
Methods: A 53-year-old female with situs inversus totalis complicated by ostium primum defect post-surgical correction with coronary artery bypass graft in infancy, atrial fibrillation, and recurrent acute pancreatitis who presented for 6 days of nausea, vomiting, and oral intolerance. Imaging demonstrated acute pancreatitis with intrahepatic and extrahepatic biliary duct dilatation, hydropic gallbladder, and multiple hypodensities in the body and head of the pancreas. Evaluation by general surgery and advanced endoscopy determined that the gastric outlet and biliary obstructions are likely secondary to pancreatic head inflammation. Furthermore, the patient’s history of recurrent acute pancreatitis and new peripancreatic fluid collections likely demonstrates disease progression to chronic pancreatitis. EGD with EUS was planned to further evaluate the pancreatic head collections, however, EUS was not completed due to technical complexity in the setting of duodenal obstruction from external compression and altered SIT anatomy. Repeat imaging after failed EUS showed a developing 4.4 cm necrotic pancreatic head mass. Patient was discharged with follow up EUS planned for further evaluation of pancreatic lesions. Discussion: Patients with situs inversus totalis are often asymptomatic with diagnosis typically occurring incidentally. Invasive surgical procedures are often challenging as structures are found in their contralateral position. This proves to be especially challenging for advanced endoscopic procedures such as ERCP and EUS. These procedures often require modified patient positioning and altered endoscopic maneuvers in the duodenum to visualize key landmarks. These adjustments can make it challenging to achieve canulation during ERCP and adequate sonographic visualization and positioning during EUS. Furthermore, the risk of iatrogenic injury is increased due to unfamiliar orientation. Imaging prior to endoscopic imaging is important to allow for endoscopic planning.