Mohannad Bitar, MD1, Mushfiqur Siddique, MD1, Sajieh Naddaf, MD1, Hasan Al-Obaidi, MD2, Hayder Alamily, MD3 1Jamaica Hospital Medical Center, Jamaica, NY; 2University of Toledo College of Medicine and Life Sciences, Toledo, OH; 3University of Colorado Anschutz Medical Campus, Denver, CO Introduction: PPP syndrome (Pancreatitis, Panniculitis, Polyarthritis) is a rare disorder with fewer than 70 cases reported. It presents as a triad of polyarthritis with intraosseous fat necrosis, lobular panniculitis, and pancreatitis (acute, chronic, or malignant). It results from systemic release of pancreatic enzymes, particularly lipase, leading to fat necrosis and inflammation in joints and subcutaneous tissues. Most patients are males in their 40s–70s with a history of alcohol use and pancreatitis. The condition carries high morbidity and mortality, particularly when associated with pancreatic malignancy.
Case Description/
Methods: A 72M with chronic pancreatitis, EtOH use disorder, and prostate cancer presented with acute pancreatitis, confirmed by elevated lipase and CT showing a pancreatic duct stone. He improved with IV fluids and was discharged. Weeks later, he returned with severe toe/knee pain, swelling, and nodular skin lesions. Rheumatology was consulted for concern of inflammatory arthritis and panniculitis. Arthrocentesis showed mildly inflammatory fluid without crystals. Migratory polyarthritis, nodules, and pancreatic disease raised concern for PPP syndrome. Imaging showed necrotic collections and pseudocysts. IV steroids were started; endoscopic drainage and stenting were performed. He developed complications, including infection, C. difficile colitis, and sepsis, requiring antibiotics, antifungals, and TPN. Despite temporary improvement, he had worsening peripancreatic collections with fistula and abscess formation, leading to septic shock and encephalopathy. Care was transitioned to comfort measures, and he ultimately passed away. Discussion: PPP syndrome is a severe and underrecognized complication of pancreatic disease. Diagnosis is clinical, supported by the classic triad and exclusion of other causes. In this case, the syndrome was diagnosed based on characteristic joint, skin, and pancreatic involvement, alongside supportive lab and imaging findings. Conservative management often fails; surgical intervention may be curative if anatomical defects like fistulas are identified. Early recognition and targeted treatment are critical, but even then, outcomes remain poor. This case highlights the need for vigilance in patients with pancreatitis presenting with systemic inflammatory symptoms.
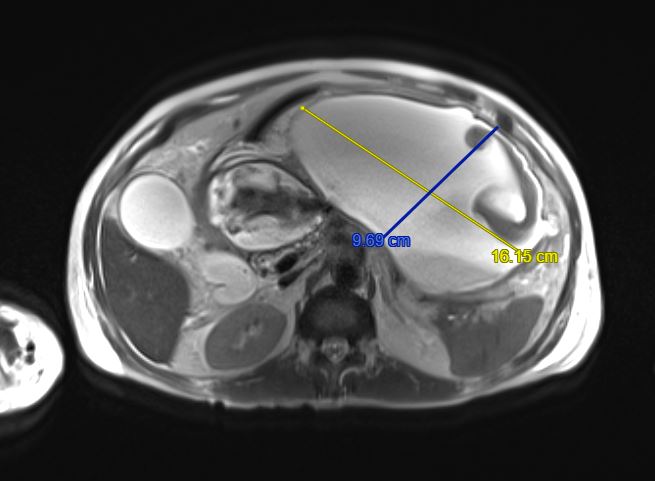
Figure: 16.2 cm peripancreatic fluid collection secondary to chronic pancreatitis
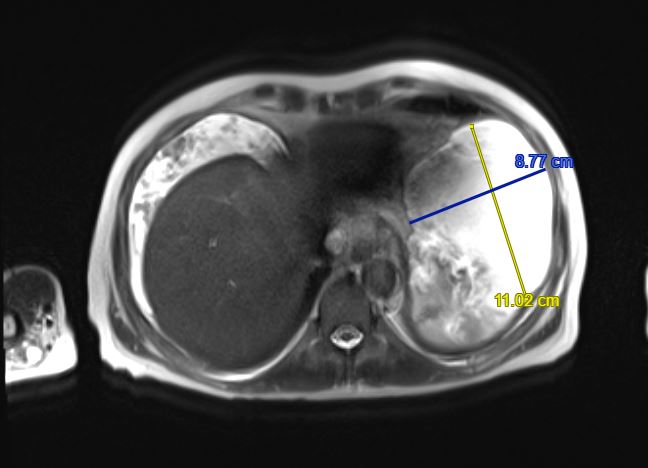
Figure: 11 cm peripancreatic fluid collection secondary to chronic pancreatitis
Disclosures: Mohannad Bitar indicated no relevant financial relationships. Mushfiqur Siddique indicated no relevant financial relationships. Sajieh Naddaf indicated no relevant financial relationships. Hasan Al-Obaidi indicated no relevant financial relationships. Hayder Alamily indicated no relevant financial relationships.
Mohannad Bitar, MD1, Mushfiqur Siddique, MD1, Sajieh Naddaf, MD1, Hasan Al-Obaidi, MD2, Hayder Alamily, MD3. P0235 - Triple the Trouble: Unraveling the Mystery of PPP Syndrome (Pancreatitis, Panniculitis, and Polyarthritis) - A Case Report, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.