Enayat Shahidifar, MD1, Carl Manzo, MD2, Marlena Lesniowska, MD1, Arman Hemmat, MD1, Timothy Barreiro, DO, MPH1 1St. Elizabeth Youngstown Hospital, Youngstown, OH; 2Mercy Health, Youngstown, OH Introduction: Biliary cast syndrome (BCS) is a rare condition characterized by intraductal casts causing biliary obstruction and cholestasis. While first described in liver transplant recipients, it is increasingly recognized in critically ill, non-transplant patients. Secondary sclerosing cholangitis in critically ill patients (SSC-CIP) is a progressive biliary injury commonly triggered by ischemia, bile stasis, and infection, with drug-induced liver injury potentially exacerbating the course. We present a rare case of BCS and SSC-CIP in a young, non-transplant patient following trauma and amputation.
Case Description/
Methods: A 39-year-old man with metabolic syndrome (BMI 47), CKD, and non-ischemic cardiomyopathy sustained a traumatic leg fracture complicated by compartment syndrome and popliteal artery injury. He underwent vascular bypass, serial debridements, and right above-knee amputation. His ICU course was complicated by ARDS, ventilator-associated pneumonia, and surgical site infections with VRE and XDR Acinetobacter, requiring prolonged treatment with hepatotoxic agents (linezolid, daptomycin). Five months later, he developed jaundice and pruritus. MRCP showed intrahepatic ductal dilation and wall thickening. Liver biopsy demonstrated cholestasis, bile infarcts, ductular reaction, and macrovesicular steatosis (35–40%) without fibrosis. Autoimmune and viral workup was negative. ERCP revealed long, fibrous biliary casts consistent with BCS, which were extracted with balloon sweep. Biliary stenting was performed, and a subsequent ERCP addressed hemobilia from an ulcerated ampulla. Discussion: This case highlights multifactorial SSC-CIP triggered by ischemia, bile stasis, and infection, with hepatotoxic antibiotics possibly aggravating bile duct injury. Histology ruled out congestive hepatopathy and confirmed SSC-CIP. Though ERCP provided temporary improvement, persistent MRSA bacteremia and poor functional status precluded liver transplant, the only definitive therapy for SSC-CIP. Clinicians should maintain a high suspicion for SSC-CIP in ICU survivors with cholestasis. Early recognition may improve outcomes, but the prognosis remains poor without transplant.
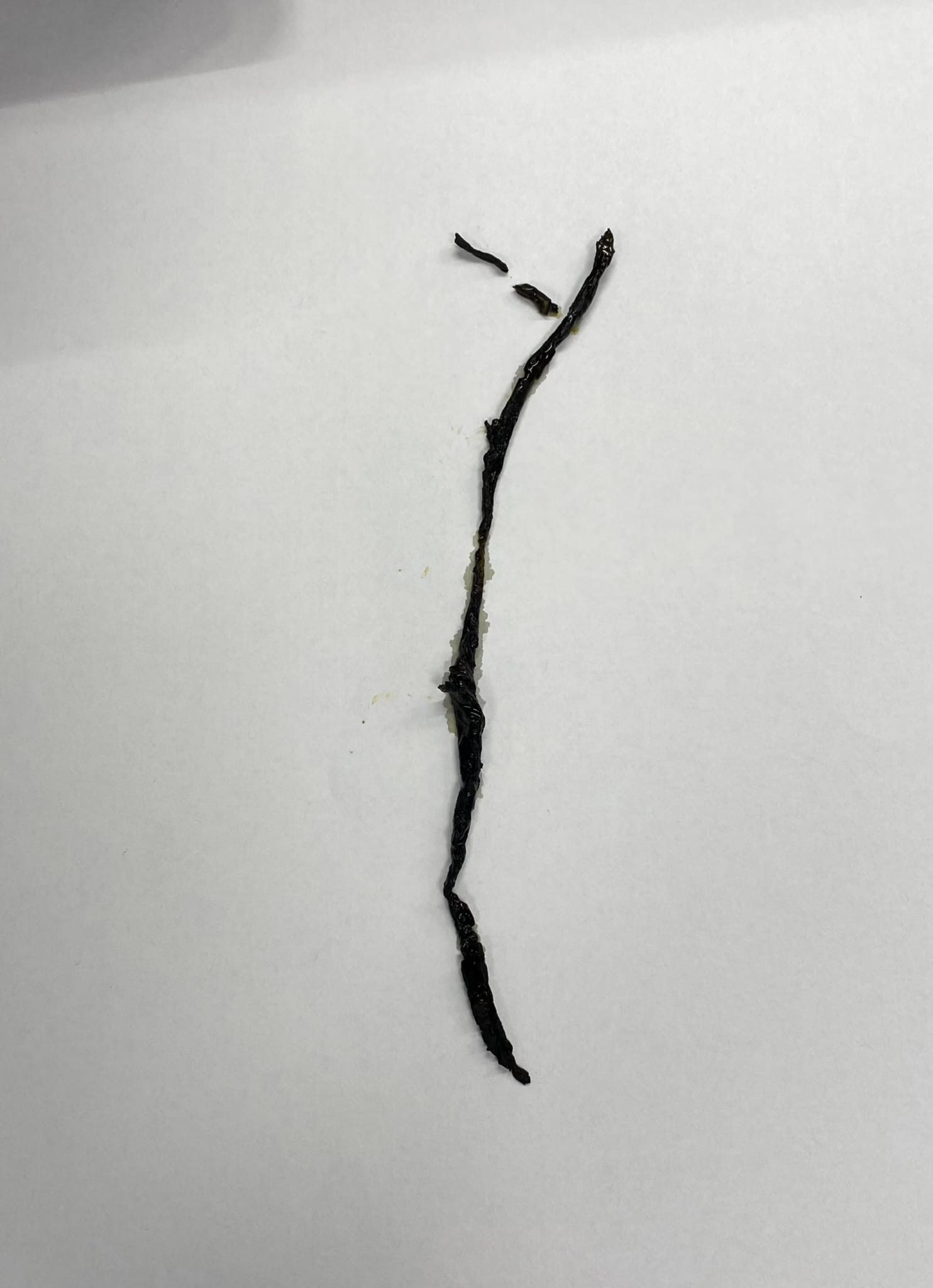
Figure: Gross specimen of a biliary cast extracted during ERCP, demonstrating a long, dark, fibrous structure conforming to the shape of the intrahepatic bile ducts. The cast morphology is consistent with biliary cast syndrome (BCS) in the setting of secondary sclerosing cholangitis in a critically ill patient.
Disclosures: Enayat Shahidifar indicated no relevant financial relationships. Carl Manzo indicated no relevant financial relationships. Marlena Lesniowska indicated no relevant financial relationships. Arman Hemmat indicated no relevant financial relationships. Timothy Barreiro indicated no relevant financial relationships.
Enayat Shahidifar, MD1, Carl Manzo, MD2, Marlena Lesniowska, MD1, Arman Hemmat, MD1, Timothy Barreiro, DO, MPH1. P0188 - Biliary Cast Syndrome and Secondary Sclerosing Cholangitis Following Trauma and Amputation in a Young Patient With Metabolic Syndrome, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")