Jacob C. Jones, DO, William M. LaShomb, MD, Jerome C. Edelson, MD Brooke Army Medical Center, San Antonio, TX Introduction: Pancreatic alpha cell hyperplasia (ACH) is a rare condition characterized by islet cell hyperplasia and significant hyperglucagonemia without glucagonoma syndrome. It is caused by inactivating GCGR mutations or sequalae of pancreatitis. Often associated with MEN-1 and pancreatic neuroendocrine tumors (NET) in later life. Here we describe a case of symptomatic diffuse pancreatic enlargement, later found to have features of ACH.
Case Description/
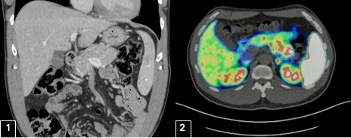
Methods: A 47-year-old male presented to the ED for months of progressive intermittent vomiting and abdominal distension. Lipase was elevated, but not >3x ULN. CT imaging was obtained which demonstrated diffuse enlargement of the pancreas with a 4cm isodense area in the pancreatic tail. [1] CA 19-9 and IgG subtypes were normal. MR imaging could not be obtained due to retained ballistic fragments. EUS revealed a diffusely enlarged pancreas with increased echogenicity and subtle echotexture change of the tail without a discrete mass. Targeted biopsies demonstrated fragments of non-atrophic pancreatic tissue with foci of bland neuroendocrine cells arranged in sheets and large nests with a ki-67 index < 3%. Immunohistochemical studies were positive for synaptophysin, INSM1, cytokeratin Cam 5.2, and chromogranin. The histologic differential included pancreatic islet cell hyperplasia, neuroendocrine microadenoma, and sampling of a well-differentiated NET.
Secretory evaluation demonstrated glucagon >1640 pg/ml. Somatostatin, chromogranin A, gastrin, VIP, glucose and A1C were normal. Out of concern for an incompletely sampled glucagonoma, repeat EUS with FNB was performed with similar pathology. The patient was referred to multi-disciplinary discussion for consideration of distal pancreatectomy, but ultimately plans were made for surveillance. Dotatate PET/CT at 5 months demonstrated increased uptake in the pancreatic tail, still without discrete mass on follow up. [2] Discussion: This case presents a complex diagnostic dilemma as alpha cell hyperplasia and glucagonoma share many features and may indeed represent the same spectrum of disease. Case reports describe both masses and positive Dotatate PET scans in ACH, further complicating the picture. It is important for physicians to include ACH in the differential when hyperglucagonemia is discovered. Optimal management is still not well defined as patients have the option of either pancreatectomy or surveillance.
Figure: 1) CT imaging demonstrating diffuse enlargement of pancreas with 4 cm isodense area in pancreatic tail. 2) Dotatate PET/CT with increased uptake in pancreatic tail.
Disclosures: Jacob Jones indicated no relevant financial relationships. William LaShomb indicated no relevant financial relationships. Jerome Edelson indicated no relevant financial relationships.
Jacob C. Jones, DO, William M. LaShomb, MD, Jerome C. Edelson, MD. P0177 - Alpha Cell Hyperplasia or Nothing but NET: A Diagnostic Dilemma, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.