Stephanie Colon-Marrero, MD, Juan G. Feliciano-Figueroa, MD, Jose Martin-Ortiz, MD, FACG VA Caribbean Healthcare System, San Juan, Puerto Rico Introduction: Mirizzi syndrome is a rare complication of gallstone disease, characterized by external compression of the common bile duct (CBD) by a large, impacted stone in Hartmann’s pouch or the cystic duct. It classically presents with obstructive jaundice; however, atypical cases without jaundice can pose significant diagnostic challenges, particularly when chronic abdominal pain is the primary symptom. Moreover, its occurrence in a gallbladder remnant post-cholecystectomy is exceptionally uncommon.
Case Description/
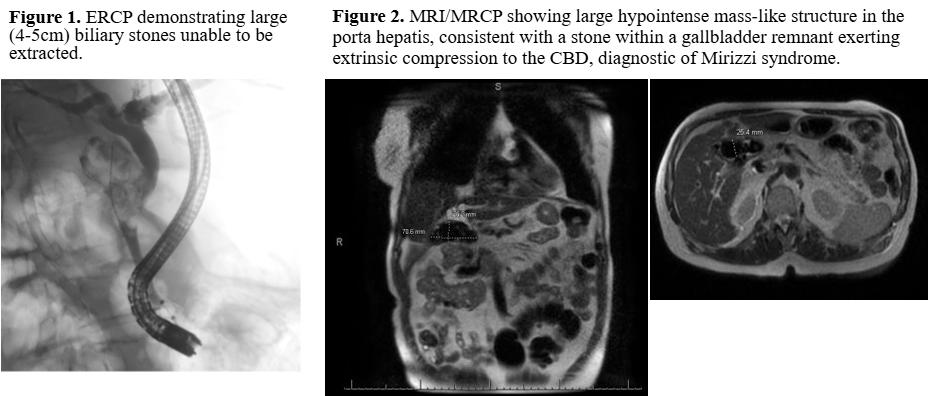
Methods: A 74-year-old male with history of hypertension, type 2 diabetes, and cholecystectomy presented with chronic post prandial abdominal pain. Imaging revealed intrahepatic and extrahepatic biliary duct dilatation with the CBD measuring 12.8 mm. Endoscopic retrograde cholangiopancreatography (ERCP) showed multiple large biliary stones (4-5 cm). Despite sphincterotomy, stone extraction was unsuccessful, and a plastic stent was placed for decompression. Liver chemistries remained cholestatic, prompting further evaluation with magnetic resonance cholangiopancreatography (MRCP). Imaging revealed a large hypointense mass-like structure in the porta hepatis, consistent with a stone within gallbladder remnant exerting extrinsic compression to the CBD, diagnostic of Mirizzi syndrome. It also showed a dislodged plastic stent in the hepatic flexure. He was discharged with surgical planning underway. Two months later, he returned with sepsis secondary to ascending cholangitis. He was treated with intravenous antibiotics and underwent a new ERCP with balloon dilation and biliary drainage. He ultimately underwent open common bile duct exploration and hepatic-jejunostomy. Postoperative recovery was uneventful, and his symptoms resolved without complications. Discussion: This case highlights an atypical presentation of Mirizzi syndrome in the absence of jaundice, which delayed the recognition of significant biliary obstruction. While ERCP successfully decompressed the biliary system initially, the unresolved mechanical obstruction remained ultimately leading to cholangitis. The occurrence of Mirizzi syndrome in a gallbladder remnant without jaundice is exceptionally rare and may mimic benign biliary conditions. Clinicians should maintain with a high index of suspicion in post-cholecystectomy patients with persistent biliary symptoms and when imaging reveals residual gallbladder tissue or cystic duct remnant. In these patients, timely surgical intervention is essential to prevent serious complications.
Figure: Biliary stone within a gallbladder remnant exerting extrinsic compression to the common bile duct, diagnostic of Mirizzi syndrome.
Disclosures: Stephanie Colon-Marrero indicated no relevant financial relationships. Juan G. Feliciano-Figueroa indicated no relevant financial relationships. Jose Martin-Ortiz indicated no relevant financial relationships.
Stephanie Colon-Marrero, MD, Juan G. Feliciano-Figueroa, MD, Jose Martin-Ortiz, MD, FACG. P0170 - Beyond the Stones: Diagnosing Mirizzi Syndrome in the Absence of Jaundice, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")