Aziz Eshov, DO1, Samit Datta, MD2 1Skagit Regional Hospital, Arlington, WA; 2Skagit Regional Hospital., Mount Vernon, WA Introduction: Post ERCP sphincterotomy bleeding (PESB) is an uncommon complication of ERCP, with incidence rates of 2%. While most cases of PESB resolve spontaneously, a minority necessitate endoscopic intervention. Hemostatic powder (HP) has emerged as a promising treatment option for active UGI bleeds. However, the adverse effects associated with HP remain poorly characterized. This is a case of a patient who developed complications following the application of HP.
Case Description/
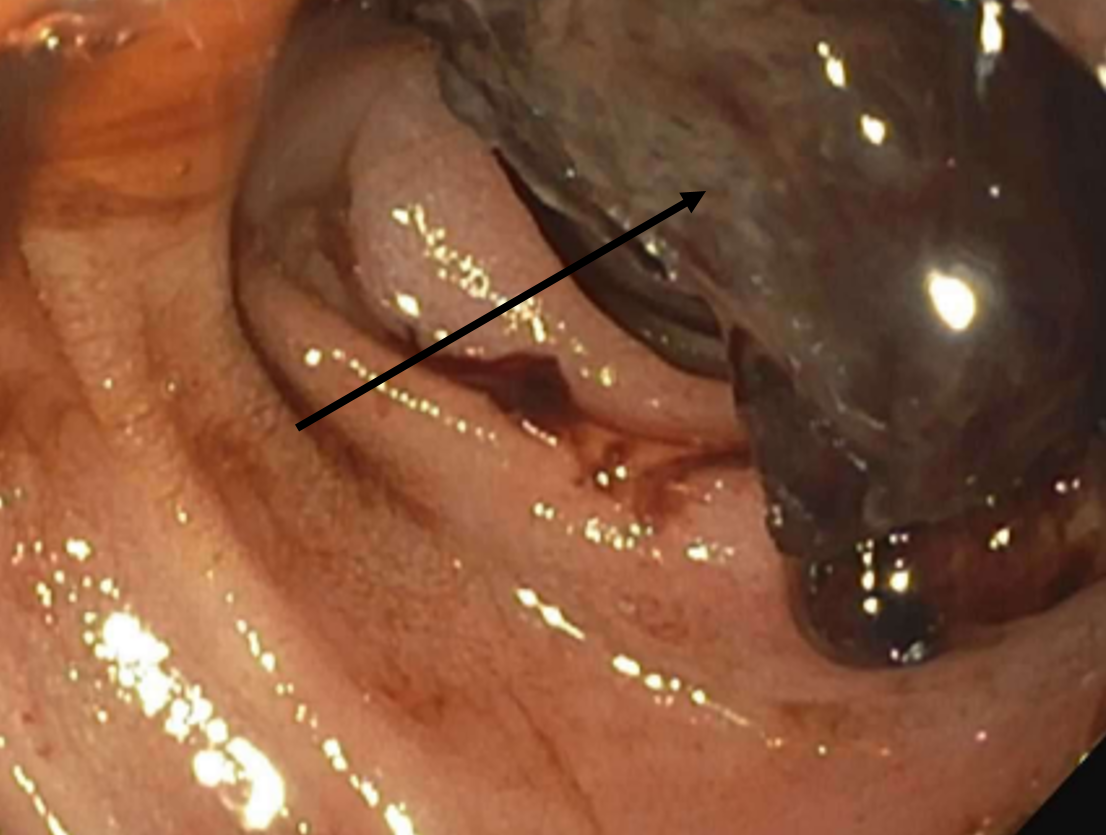
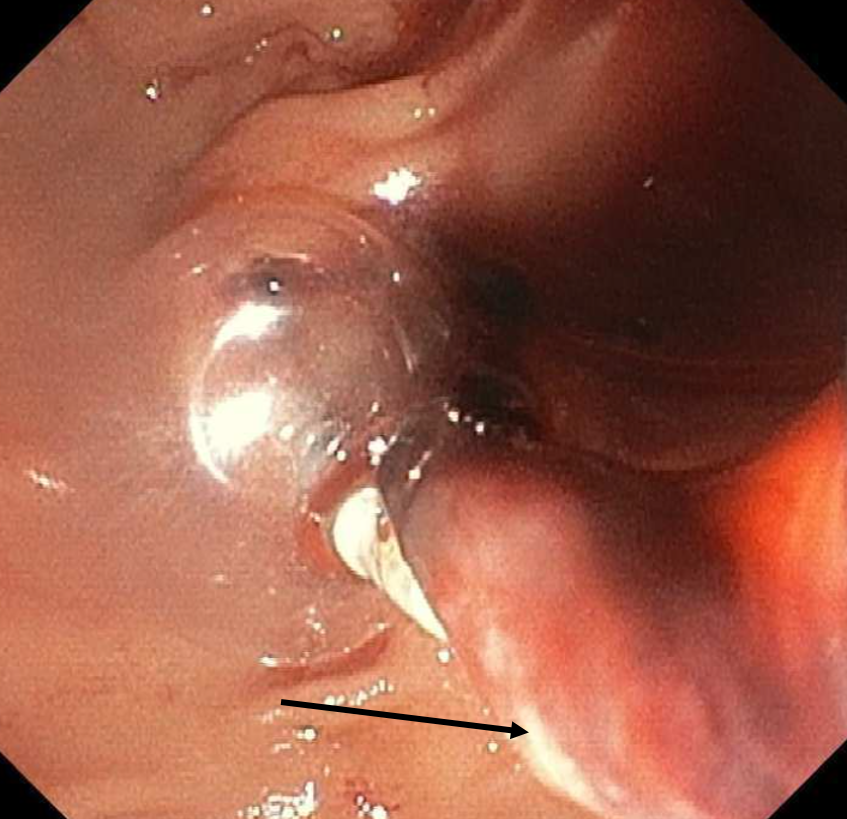
Methods: A 71-year-old female presented with obstructive jaundice. A CT scan of the abdomen revealed cholelithiasis. MRCP showed choledocholithiasis and ERCP with sphincterotomy revealed mild bile duct stenosis, which was addressed with dilation. 2 days post-procedure, patient developed melena, and CTA abdomen showed extravasation in the duodenum. An urgent EGD revealed clots around the sphincterotomy site, and hemostasis was achieved using HP and endoclips. Bilirubin subsequently trended up to 7.3 and patient had repeat ERCP with findings of sludge and pus. A biliary stent was placed for decompression. Patient improved and was discharged in stable condition. She returned 1 day later with abdominal pain. A limited MRCP failed to visualize the biliary ducts and ERCP revealed large clots (Figure 1) without evidence of the previously placed endoclips or stents. A balloon sweep of the duct encountered resistance during the pull phase, producing clots mixed with white debris without obvious pus, raising suspicion for HP-induced biliary obstruction (Figure 2). Fully covered metal stent was placed. Despite these interventions, the patient's condition continued to decline due to overwhelming sepsis and she passed away. Discussion: PESB is a rare complication that often resolves spontaneously. However, in severe cases, endoscopic intervention may be necessary. Management of PESB includes epinephrine injection, endoclips, plasma cautery, and IR embolization. HP has emerged as a promising option for managing UGI bleeds, but its adverse events have not been studied. In our case, patient developed a biliary duct obstruction due to HP. Of note, our patient had pre-existing, idiopathic biliary strictures. While cholangioscopy would have helped confirm if there was residual HP in the CBD, our recommendation based on this case report would be to avoid HP in the management of PESB.
Figure: Figure 1. Large duodenal clot (arrow).
Figure: Figure 2. Mix of hemostatic powder with blood clots at the end of balloon sweep (arrow).
Disclosures: Aziz Eshov indicated no relevant financial relationships. Samit Datta indicated no relevant financial relationships.
Aziz Eshov, DO1, Samit Datta, MD2. P0165 - Biliary Duct Obstruction Following Hemospray Application for Sphincterotomy Bleeding Complication, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.


 photo")