Anas Al Mardini, MBBS1, Praneeth Jasti, MBBS2, Husein Abu-Rumman, MD3, Canan D. Dirican, MD4, John Devereux, 5 1NYMC at St Mary's and St Clare's, Montclair, NJ; 2NYMC St Mary's, St Clare's hospital, Montclair, NJ; 3NYMC St Mary, St Clare hospital, Paterson, NJ; 4NYMC at St Mary's and St Clare's, Denville, NJ; 5Saint Clare's Health, New York Medical College, Denville, NJ Introduction: Biloma is an encapsulated collection of bile outside the biliary tree, typically resulting from trauma, iatrogenic injury, or biliary obstruction. While uncommon, with an incidence ranging from 0.3% to 2%, bilomas can lead to significant morbidity if not promptly diagnosed and managed. The most frequent etiology of biloma is iatrogenic injury during surgical procedures such as cholecystectomy or ERCP. Other causes include abdominal trauma, choledocholithiasis, and spontaneous rupture of hepatic cysts. Clinically, patients may present with right upper quadrant pain, jaundice, and fever, though symptoms can be nonspecific, complicating diagnosis. Imaging modalities such as ultrasound, CT, and MRI are pivotal in diagnosing bilomas and assessing their relationship with adjacent structures. Management strategies vary based on the size and symptoms of the biloma, ranging from conservative observation to percutaneous drainage or surgical intervention. This report presents a case of recurrent biloma following cholecystectomy, aiming to contribute to the understanding of this rare condition and its management.
Case Description/
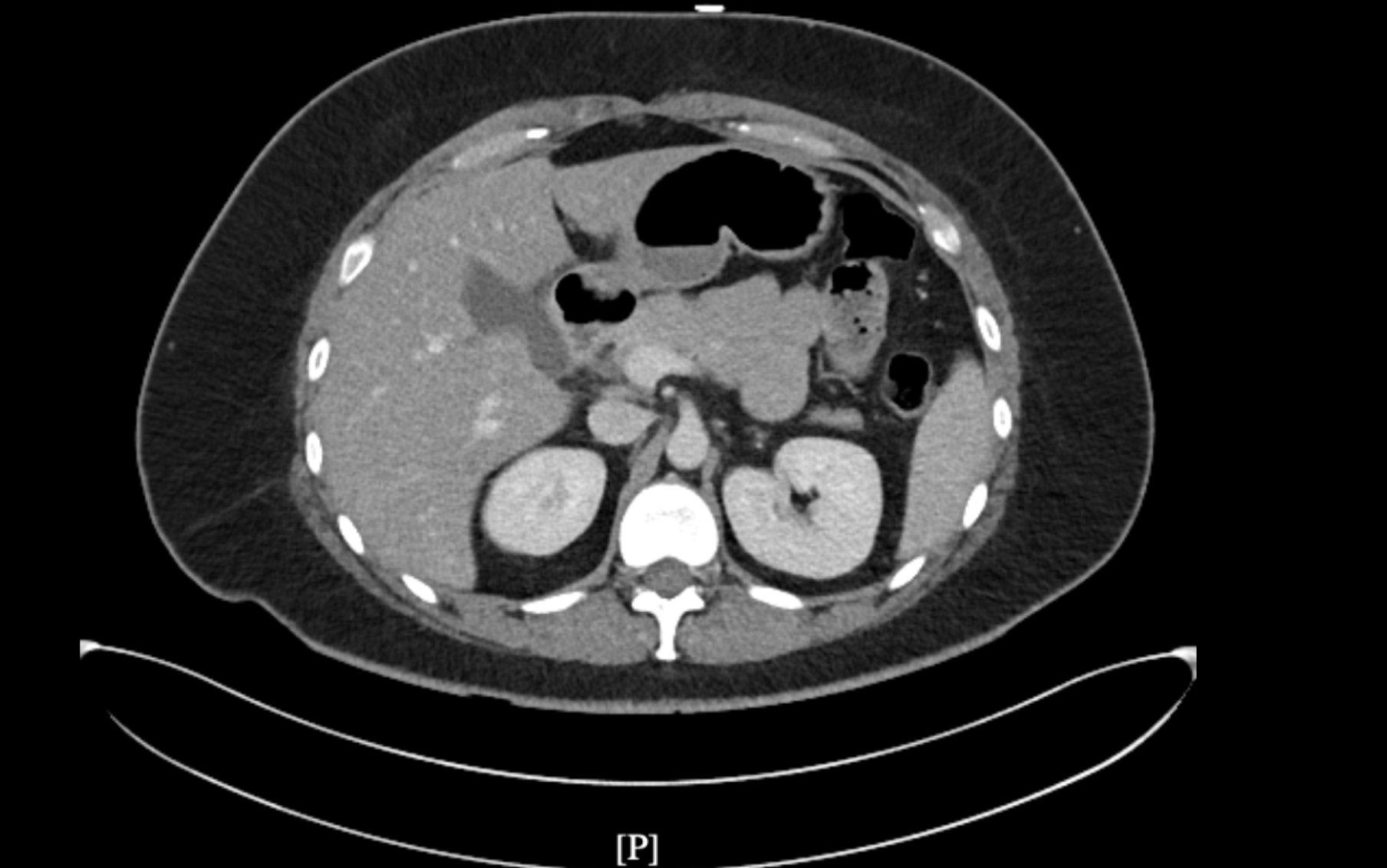
Methods: 28-year-old female with past surgical history of cholecystectomy, presented with severe, intermittent RLQ abdominal pain radiating to the upper quadrant. Abdomen CT scan revealed a 6.5 cm fluid collection in the gallbladder fossa, consistent with a biloma. The patient underwent CT-guided percutaneous drainage of the fluid collection, with 75 cc aspirated and a Jackson-Pratt (JP) drain placed, resulting in partial symptom relief. Subsequently she underwent ERCP, which demonstrated a normal biliary tree and an intact cystic duct stump, with no extravasation of contrast. A CBD stent was placed. Despite these interventions, the patient developed persistent abdominal pain accompanied by nausea and vomiting. Laboratory evaluation revealed an elevated lipase level, and a diagnosis of post-ERCP pancreatitis was made. She was managed conservatively with bowel rest, NPO, intravenous fluids, pain control, and early ambulation. Her symptoms improved within 48 hours. The patient was discharged with drain in situ. At follow-up after 10 days, repeat CT imaging showed resolution of the fluid collection, and the JP drain was removed. The CBD stent was subsequently removed after approximately 2 months Discussion: While biloma can be a complication after cholecystectomy or ERCP, denovo recurrent biloma can occur and we should have a high index of suspicion in order to make the diagnosis.
Figure: 7*2.2*2.2 cm fluid collection in the gallbladder fossa (Biloma)
Disclosures: Anas Al Mardini indicated no relevant financial relationships. Praneeth Jasti indicated no relevant financial relationships. Husein Abu-Rumman indicated no relevant financial relationships. Canan Dirican indicated no relevant financial relationships. John Devereux indicated no relevant financial relationships.
Anas Al Mardini, MBBS1, Praneeth Jasti, MBBS2, Husein Abu-Rumman, MD3, Canan D. Dirican, MD4, John Devereux, 5. P0100 - Recurrent Biloma Post Cholecystectomy: Diagnostic and Therapeutic Challenges, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")