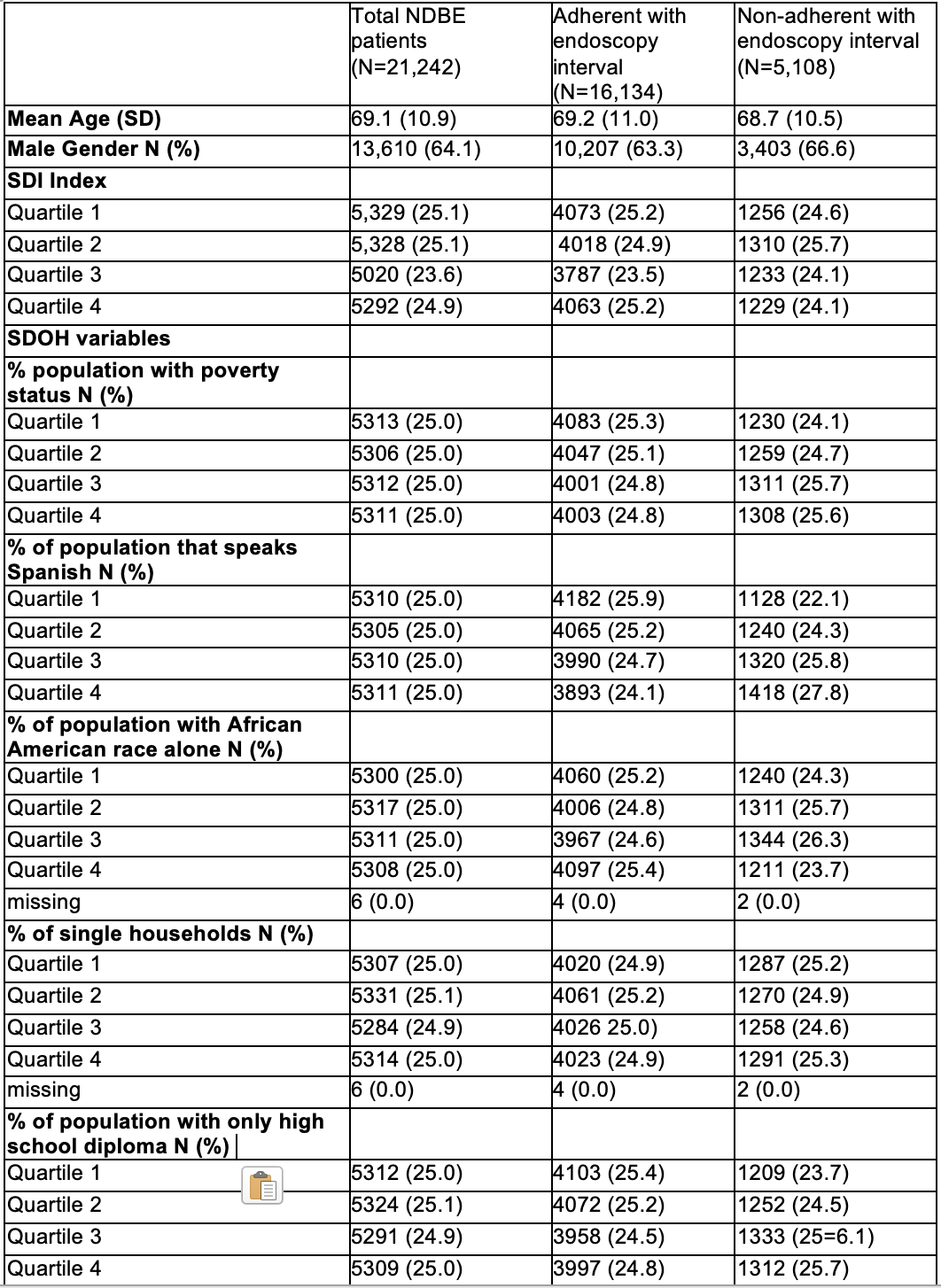
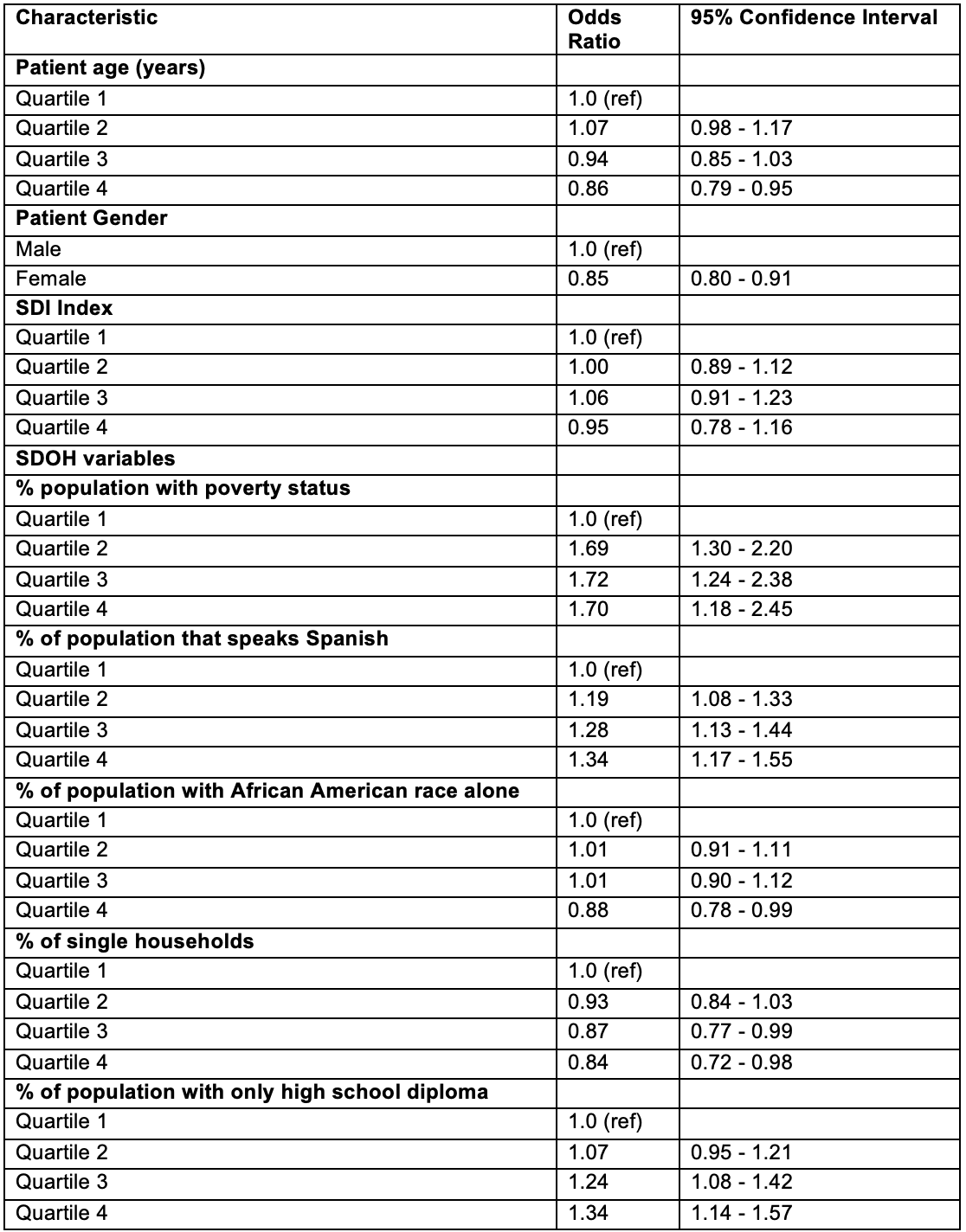
Lovekirat Singh Dhaliwal, MD1, Jennifer Holub, MPH2, Saurabh Chawla, MD, FACG3, Prasad Iyer, MD, MS4, Allon Kahn, MD, FACG5 1Emory University School of Medicine, Decatur, GA; 2GI Quality Improvement Consortium, Ltd., North Bethesda, MD; 3Emory University School of Medicine, Atlanta, GA; 4Mayo Clinic, Phoenix, AZ; 5Mayo Clinic College of Medicine and Science, Scottsdale, AZ Introduction: Barrett’s esophagus (BE) progresses from non-dysplastic BE (NDBE) to esophageal adenocarcinoma (EAC) through dysplasia, with surveillance aiming to detect dysplasia early and prevent progression. Despite guidelines, adherence to surveillance remains suboptimal, potentially due to patient barriers and racial or socioeconomic disparities. We aimed to explore the impact of SDOH on adherence to surveillance endoscopy for NDBE surveillance using the GI Quality Improvement Consortium (GIQuIC) registry. Methods: Patients with a confirmed diagnosis of NDBE in the GIQuIC registry (2013–2023) and at least one follow-up endoscopy were included. Adherence to surveillance was defined as follow-up endoscopy within 6 months of recommended intervals. SDOH data and Social Deprivation Index were linked by ZIP code and combined with clinical data to evaluate their impact on surveillance adherence. A logistic regression model with backward selection was used, with the p-value threshold optimized based on AUC performance. Model validation was performed using a held-out 20% sample. Results: We identified 103,601 patients with NDBE, of whom 21,242 underwent repeat endoscopy; 75.9% (N=16,134) were adherent to surveillance recommendations. Baseline characteristics are shown in Table 1. Factors associated with non-adherence (Table 2) include higher area-level poverty (Q1 vs Q4 OR 1.70, 95% CI 1.18–2.45), greater proportion of Spanish-speaking residents (OR 1.34, 95% CI 1.17–1.55), and lower educational level (OR 1.34, 95% CI 1.14–1.57). Adherence was more likely among older patients (OR 0.86, 95% CI 0.79-0.95), females (OR 0.85, 95% CI 0.80–0.91) and in areas with a higher percentage of African American residents (OR 0.88, 95% CI 0.78–0.99). Discussion: Adherence to NDBE surveillance is significantly influenced by social determinants such as poverty, language barrier, and education level. Notably, economic disparities may have a greater impact than racial disparities. These findings underscore the importance of addressing socioeconomic barriers to improve surveillance adherence, particularly in underserved populations.
Figure: Table 1: Baseline characteristics of patients
Figure: Table 2: Factors associated with non-adherence to follow-up endoscopy
Disclosures: Lovekirat Singh Dhaliwal indicated no relevant financial relationships. Jennifer Holub indicated no relevant financial relationships. Saurabh Chawla indicated no relevant financial relationships. Prasad Iyer: CDx medical – Consultant, Grant/Research Support. Exact – Grant/Research Support. Exact Sciences – Consultant, Grant/Research Support. Medtronic – Consultant. Pentax Medical – Consultant, Grant/Research Support. Allon Kahn: MiMedx – Consultant.
Lovekirat Singh Dhaliwal, MD1, Jennifer Holub, MPH2, Saurabh Chawla, MD, FACG3, Prasad Iyer, MD, MS4, Allon Kahn, MD, FACG5, 1, Impact of Social Determinants of Health in Non-Dysplastic Barrett’s Esophagus Surveillance: An Analysis Using the GIQuIC Database, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.





 photo")